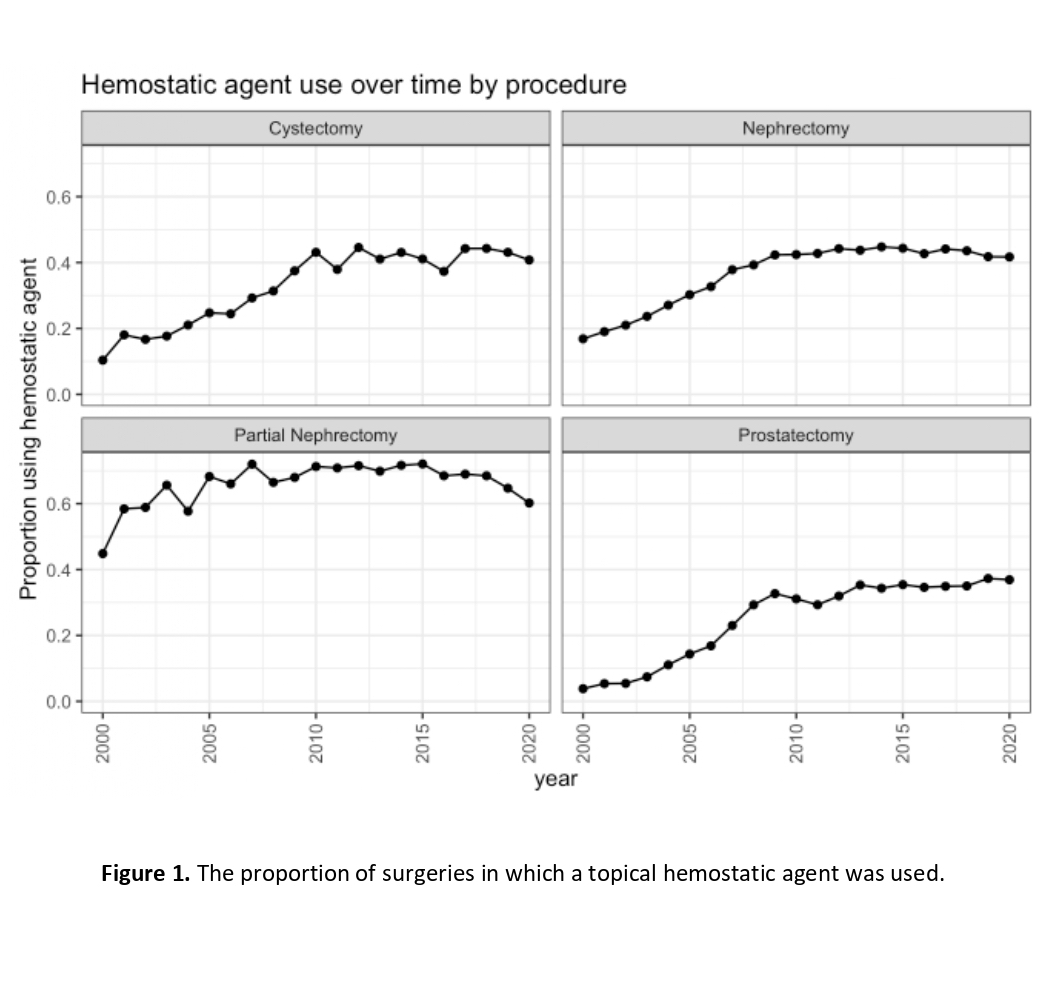
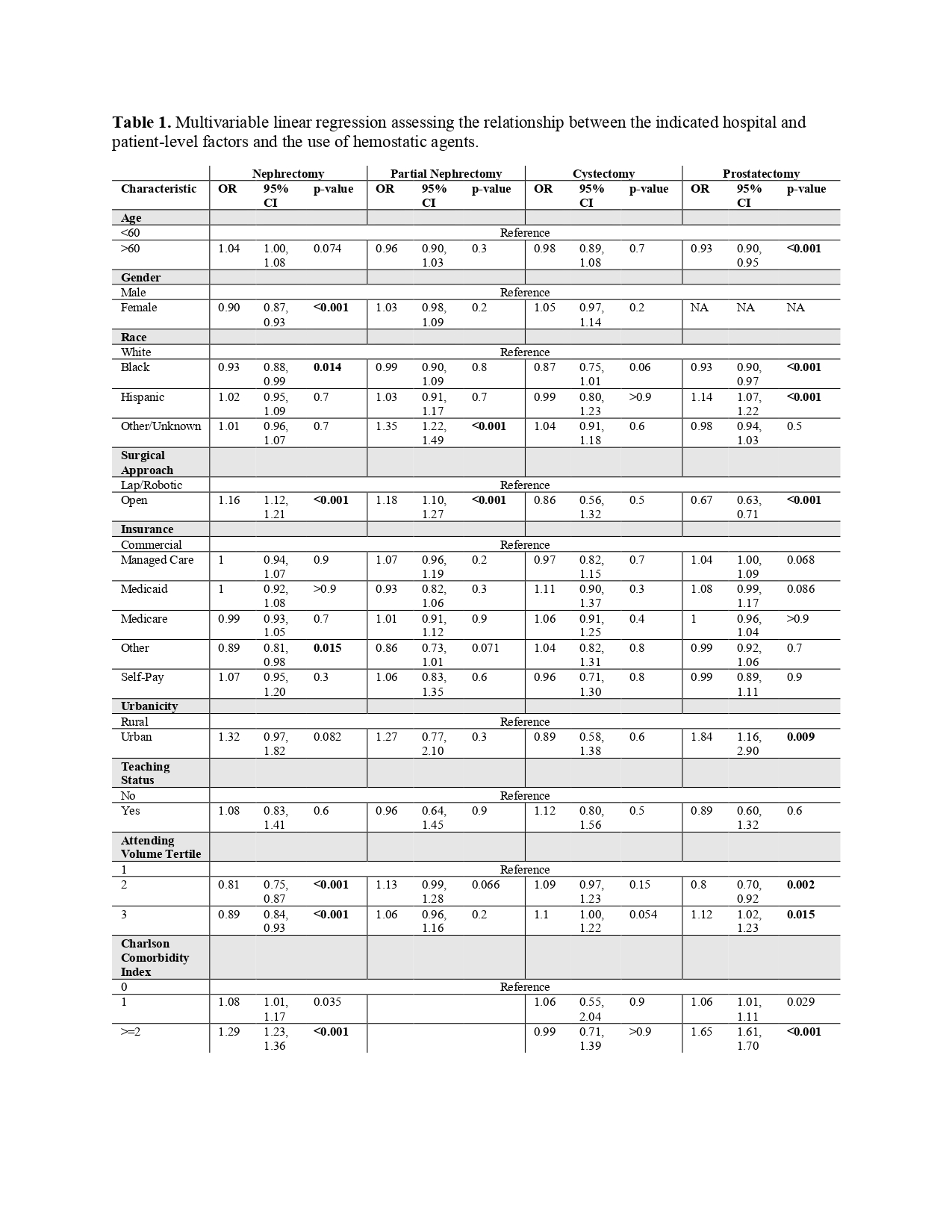
Introduction: Hemostatic agents are used to prevent hemorragic complications in surgeries. The national trends in the use and the cost associated with these agents in major urologic procedures are largely unknown. Methods: This retrospective US analysis used the Premier Healthcare database. Patterns of hemostatic agent use in major urologic surgeries were investigated and correlated with patient and hospital characteristics over the past two decades. Multivariable mixed-effects logistic regression was used to identify predictors of hemostatic agent use. Results: The final patient cohort included 385,261 patient encounters for urologic surgery from 2000 to 2020. In 2020, hemostatic agents were used in 36.91% of prostatectomies, 41.69% of radical nephrectomies, 60.22% of partial nephrectomies and 40.77% of cystectomies. In the multivariable models, For patients undergoing prostatectomy odds for receiving hemostatic agent was 14% higher in Hispanic men (OR 1.07, CI 1.22- 1.24; P<0.001) and 7% lower in Black patients men (OR 0.93, CI 0.90- 0.97; P<0.001), 33% lower for open surgery compared to laparoscopic/robotic approach (OR 0.67, 95% CI 0.63- 0.71; P<0.001). For radical nephrectomy patients, odds of receiving hemostatic agent were 16% higher for open approach (OR 1.16, 95% CI 1.12- 1.21; P<0.001), 7% lower for Black race (OR 0.93, 95% CI 0.88- 0.99; P 0.014). For partial nephrectomy patients odds for receiving hemostatic were 18% higher for open approach (OR 1.18, 95% CI 1.10- 1.27; P<0.001). The specific cost for hemostatic use did not differ between lap/robotic and open approaches for any procedure. Conclusions: The use of hemostatic agents has increased markedly in the last decade. Patient characteristics, surgeon, and hospital factors are highly associated with the use of hemostatic agents. Specific costs of the hemostatic and the proportion of the total cost of hospitalization have increased. There is a great need to develop controlled clinical trials capable of demonstrating the true efficacy of hemostatic agents to determine their specific indications. SOURCE OF Funding: J.E.S is supported by the Frederick J. and Theresa Dow Fund of the New York Community Trust, the Vinney Scholars Award, and a Damon Runyon Cancer Research Foundation Physician-Scientist Training Award.

 photo")