Research Associate Translational Oncology and Urology Research (TOUR), King’s College London, London, UK London, United Kingdom
Introduction: Renal cell carcinoma (RCC) represents 2.2% of all new cancers worldwide. Outcomes are reported inconsistently with variability in definition and measurement. Numerous EAU RCC guideline panel commissioned systematic reviews have encountered this problem. The impact is that it is difficult to compare intervention effectiveness and synthesise outcomes for guidelines. The downstream clinical relevance is uncertainty in the evidence to guide patient-clinician decision-making. A solution is a core outcome set (COS) (an agreed minimum set of outcomes). We aimed to describe the extent of outcome reporting, definitions, and measurement heterogeneity as the first stage of co-creating a COS for localised kidney cancer, using a multi-stakeholder approach.
Methods: We systematically reviewed 2785 studies (RCTs, cohort studies, case control studies, systematic reviews) up to June 2020 which met our inclusion criteria. Case studies were excluded. Abstracts and full texts were screened independently by two reviewers and in case of disagreement, a third reviewer was involved. Data extractions were double checked.
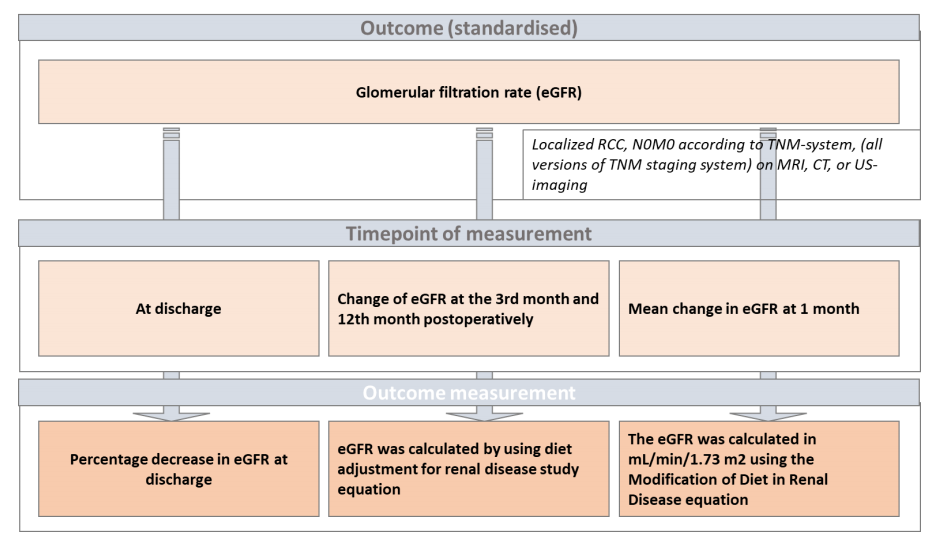
Results: 155 studies were included. The most frequently reported outcomes were linked to surgery (n= 192) (e.g. operation time, estimated blood loss, clamping time). Next most common outcomes reported were complications (n= 105) and estimated Glomerular Filtration Rate (eGFR) (n=86), followed by overall survival (n=78) and cancer-specific survival (n= 66). Definitions were heterogeneous, e.g., eGFR measurements (Figure 1). Only two studies reported outcomes linked to health related quality of life.
Conclusion: Patients, key stakeholders as the recipients of care, are not well served by the current evidence base on outcomes that reflect patient experience to inform treatment decision-making. Outcome reporting is characterised by disparate definitions and measurement heterogeneity in localised kidney cancer research. EGFR is highlighted to exemplify the difficulty of combining data from disparate definitions. Reporting, definition, and measurement heterogeneity makes evidence syntheses cumbersome and uninformative for guideline development. Furthermore, there is a dearth of PROMs, yet an overabundance of surgical parameter outcomes reported in RCC research.