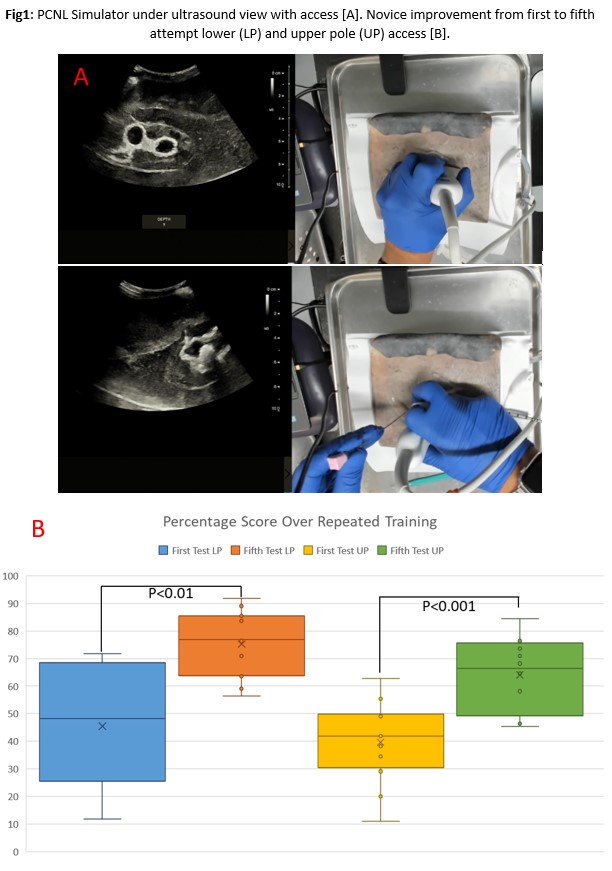
PD01-05: Multicenter validation of a consensus-based hydrogel simulator for ultrasound guided percutaneous nephrolithotomy using modern education theory.
Introduction: Ultrasound-guided approaches for percutaneous nephrolithotomy (US-PCNL) offer several advantages, including significant reduction in radiation exposure; however, they have not been readily adapted. Some of the contributing factors include the lack of a standard training platform and curriculum that has been uniformly approved by experts. As such, there is a current need for a realistic simulator. Herein, we used a consensus-based educational approach for development and multicenter validation of a high-fidelity non-biohazardous PCNL simulator. Methods: Consensus was reached on a high-fidelity PCNL simulator with 12 international experts using a Delphi methodology over three rounds. The 284 questions were categorized into overall utility, anatomical components, tissue fidelity, and assessment of surgical performance. A hydrogel prototype replicating mechanical properties was developed for experts to evaluate prior to its validation by comparing performances of 20 experts and 28 novices from 5 centers as well as evaluating the models ability to improve novice performance with repeated practice. Results: Consensus (>80% agreement) was reached in 31.3% of questions, within which 65% achieved 100% consensus. The prototype prone PCNL simulator included anatomical landmarks (11th and 12th rib, iliac crest), realistic external and ultrasound appearance with appropriate tactile properties, and a water tight distensible pelvicalyceal system with a stone for laser lithotripsy and retrograde ureteroscopy (Fig1A). A weighted evaluation checklist was also developed via consensus. Experts agreed that >89.2% of prototype and checklist components conformed to the consensus statement. Novices and experts were graded for US-guided lower pole access, with statistically significant differences for checklist score (42.3 ± 19.0% vs 93.4 ± 4.6%, P<0.001). Furthermore, novices significantly improved both lower pole and upper pole access score (P <0.01, P<0.001) respectively with repeated (x5) training sessions (Fig1B). Conclusions: This non-biohazardous benchtop simulator for US-PCNL developed using expert consensus and validated via an educational approach at multiple centers can provide safe, realistic training in a risk-free environment. SOURCE OF Funding: None