067 - Endovascular foam sclerosis for refractory bleeding rectal varices via a paraumbilical approach
Edward Colombo, MD – PGY-2, Northwell Health; Joseph Moirano, N/A – 4th year medical student, Hofstra Medical School; Asaph Levy, MD – Attending Physician, Northwell Health
Purpose: Interventional Radiologists perform many percutaneous endovascular interventions within the portal system. We highlight a case of rectal variceal embolization demonstrating the safety and efficacy of intervention via a paraumbilical approach.
Material and Methods: We present the case of a 75 year-old female with history of cryptogenic cirrhosis (MELD 25) and portal hypertension with extensive varices presenting with recurrent rectal bleeding refractory to endoscopic management. IR was consulted for endovascular embolization.
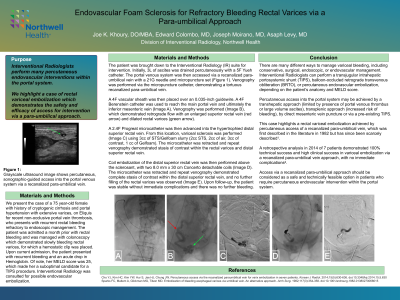
Results: Initially a paracentesis was performed. The portal venous system was accessed via a recanalized paraumbilical vein with a micropuncture set. A 4F vascular sheath was placed over an 0.035-inch guidewire. A 4F Berenstein catheter was used to reach the main portal vein and ultimately the inferior mesenteric vein (IMV). IMV venography was performed which demonstrated retrograde flow with an enlarged superior rectal vein and dilated rectal varices. A 2.4F Progreat microcatheter was then advanced into the hypertrophied distal superior rectal vein. From this location variceal sclerosis was performed using 3cc of STS/Gelfoam slurry (2cc STS, 2cc of air, 3cc of contrast, 1 cc of Gelfoam). The microcatheter was retracted and repeat venography demonstrated stasis of contrast within the rectal varices and distal superior rectal vein. Coil embolization of the distal superior rectal vein was then performed above the sclerosant with two 8.0 mm x 30 cm Concerto detachable coils. The microcatheter was retracted and repeat venography demonstrated complete stasis of contrast within the distal superior rectal vein and no further filling of the rectal varices was observed. Upon follow-up, the patient was stable without immediate complications and there was no further bleeding.
Conclusions: Percutaneous access into the portal system may be achieved by a transhepatic approach, transplenic approach, by direct mesenteric vein puncture or via a TIPS. This case highlights a rectal variceal embolization achieved by percutaneous access of a recanalized paraumbilical vein, which was first described in the literature in 1982 but has since been scarcely mentioned1. Access via a recanalized paraumbilical approach should be considered as a safe, and technically feasible option in patients who require percutaneous, endovascular intervention within the portal system.