Adam Alayli, BS – Medical Student, Morsani College of Medicine, University of South Florida; James Vogler, MD – Fellow, Vascular & Interventional Radiology, University of South Florida; Clifford Raymond, MD – Fellow, Vascular & Interventional Radiology, University of South Florida; L. Shane Grundy, MD – Affiliate Assistant Professor, Vascular & Interventional Radiology, Radiology Partners; University of South Florida; Kamal Massis, MD – Assistant Professor, Vascular & Interventional Radiology, Radiology Partners; University of South Florida; Jamil Shaikh, MD – Assistant Professor, Vascular & Interventional Radiology, Radiology Partners; University of South Florida; Glenn Hoots, MD – Assistant Professor, Vascular & Interventional Radiology, Radiology Partners; University of South Florida
Purpose: To discuss a unique case of complex semi-permanent inferior vena cava (IVC) filter removal complicated by aortic injury requiring surgical intervention. We explore strategies for removing semi-permanent and permanent filters then review potential complications and their associated management.
Material and Methods: All PHI was managed according to the HIPAA protocols at our institution. Patient history and imaging was reviewed in a standard electronic medical record and PACS workstation. The procedures described were performed using standard angiography technique. The patient was followed throughout his hospital course until discharge.
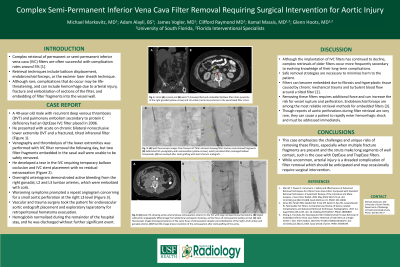
Results: A 49-year-old male with recurrent DVT and PE secondary to protein C deficiency had an OptEase IVC filter placed in 2006. He presented with acute on chronic bilateral nonocclusive lower extremity thrombus and a tilted infrarenal filter with multiple fracture fragments. Venography and thrombolysis of the lower extremities was performed with IVC filter removal the following day. Two filter fragments embedded in the caval wall were unable to be safely removed. He developed a tear in the IVC requiring temporary balloon occlusion and IVC stent placement without residual extravasation. Overnight he had continued pain and bleeding concerning for retroperitoneal bleed. He was taken for arteriogram which demonstrated active bleeding from the right gonadal, L2 and L3 lumbar arteries, which were embolized with coils. He continued to have worsening symptoms requiring large volume blood products, prompting repeat angiogram concerning for a small aortic perforation at the right L3 level. Vascular and trauma surgery took the patient for endovascular aortic endograft placement and exploratory laparotomy for retroperitoneal hematoma evacuation. His hemoglobin normalized during the remainder of his hospital stay, and he was discharged without further significant event.
Conclusions: Removal of nearly every permanent and semi-permanent filter has been described, be it intact or in piecemeal fashion. This case emphasizes the challenges and unique risks of removing these filters, especially when multiple fracture fragments are present and the struts make long segments of wall contact, such as the OptEase and TrapEase filters. While uncommon, arterial injury is a dreaded complication of filter removal which should be anticipated and may occasionally require surgical intervention.