039 - Transpleural Systemic Artery to Pulmonary Artery Shunts: A rare mimicker of Pulmonary Arteriovenous Malformations.
Shin Mei Chan, MS4 – Medical Student, Yale School of Medicine; Jeffrey Pollak, MD – Professor and Director of HHT, Interventional Radiology, Yale School of Medicine; Todd Schlachter, MD – Assistant Professor, Interventional Radiology, Yale School of Medicine
Purpose: Transpleural systemic artery to pulmonary artery shunts are a rare potential mimicker of Pulmonary Arteriovenous Malformations (PAVMs). This study describes the imaging characteristics of these lesions and discusses management.
Material and Methods: An IRB-approved retrospective medical record review of pulmonary vascular anomalies identified between January 2007 and February 2022 was performed. Patient presentation, imaging characteristics, and treatment were recorded.
Results: Eight patients with transpleural systemic artery to pulmonary artery shunts were identified. Average patient age was 48.4 years, including five males (62.5%) and three females (37.5%). History of thoracic surgery was present in five cases (62.5%) and trauma without surgery in one case (motor vehicle collision) (12.5%). The remaining two cases were presumed to be congenital (25.0%). Involvement of the inferior phrenic artery was most commonly identified (75.0%), followed by the internal thoracic (50.0%). In five cases (62.5%) the lesions were incorrectly referred for Pulmonary AVM treatment.
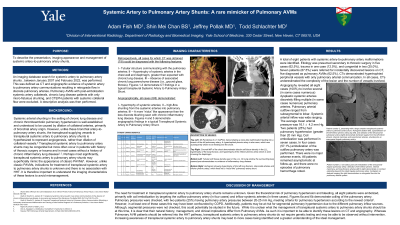
On computed tomography (CT), transpleural systemic artery to pulmonary artery shunts demonstrated the following features: I – Tubular structure communicating with the pulmonary arteries; II – Hypertrophy of systemic arteries in the chest wall and diaphragm; III – Absence of associated chronic lung parenchyma disease. Angiographically transpleural systemic artery to pulmonary artery shunts, demonstrated: I - hypertrophy of systemic arteries; II – high-flow shunting from the systemic arteries into pulmonary arteries; III – A more “nidus” like appearance than the less discrete blushing seen with chronic inflammatory lung disease.
All eight patients were treated with embolization given limited available data and theoretical risk of bleeding and pulmonary hypertension (present in two cases). Embolization was done primarily with coil embolization (in seven cases) by targeting the outflow pulmonary artery (in four cases) and inflow systemic arteries (in three cases). Technical success was 100% with no complications.
Conclusions: Transpleural systemic artery to pulmonary artery shunts are a rare potential mimicker of Pulmonary AVMs. While ideal management remains unknown, it is important to identify and distinguish these lesions from Pulmonary AVMs as the management and implications are vastly different.