006 - Computer-Aided Aspiration Thrombectomy for the Treatment of Pulmonary Embolism: Interim Analysis of the STRIKE-PE Study
Suhail Dohad, MD – TBATBATBATBATBATBATBA, Cedars-Sinai Medical Center; W. Brent Keeling, MD – Associate Professor of Surgery, Emory University School of Medicine; John Moriarty, MB, BCh – Associate Professor, David Geffen School of Medicine at UCLA; Keith Sterling, MD – Associate Professor, Inova Health System
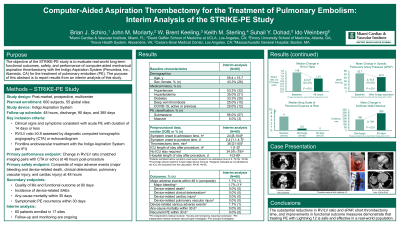
Purpose: The objective of the STRIKE-PE study is to evaluate real-world long-term functional outcomes, safety, and performance of computer-aided mechanical aspiration thrombectomy with the Indigo Aspiration System (Penumbra, Inc., Alameda, CA) for the treatment of pulmonary embolism (PE). The purpose of this abstract is to report results from an interim analysis of this study.
Material and Methods: The STRIKE-PE study is a prospective, multicenter study of adult patients with clinical symptoms consistent with acute PE of 14 days or less and a right ventricle/left ventricle (RV/LV) ratio of 0.9 or greater. This interim analysis includes patients who received frontline endovascular treatment with Lightning 12.
Results: This interim analysis includes 60 patients at 17 US sites; mean age was 59.4 years, 43.3% were female, and 95.0% had submassive PE. Median onset to admission time was 24 hours (IQR 8-104) and median admission to puncture time was 18 hours (IQR 8-27). Median baseline RV/LV ratio was 1.50 (IQR 1.26-1.79). Mean baseline systolic pulmonary artery pressure (sPAP) was 52.5 mm Hg (SD 12.3). Median thrombectomy time was 36 minutes (IQR 21-50). Of the patients with an ICU stay, the median ICU length of stay was 1 day (IQR 1-2); 19 of 55 patients (34.5%) did not require an ICU stay. Median length of hospital stay was 4 days (IQR 3-6).
One major adverse event occurred within 48 hours—an access site hematoma requiring transfusion. One device-related serious adverse event occurred. Within 30 days, no deaths or symptomatic PE recurrences occurred. The decrease in RV/LV ratio from baseline to 48 hours was 0.27 (IQR 0.17-0.59; P <.001), a reduction of 24.3%. Improvement in sPAP from before to after thrombectomy was 10.6 mm Hg (SD 10.5; P <.001), a reduction of 19.9%. The Borg dyspnea scale (range, 0-10) at rest decreased from 4 (somewhat severe; IQR 2-6) at baseline to 0.5 (very, very slight [just noticeable]; IQR 0-1) at discharge and to 0 (nothing at all; IQR 0-0.5) at 90-day follow-up. The distance covered by the 6-minute walk test increased by 103.8 meters (SD 97.3; P <.001) from discharge to 90-day follow-up.
Conclusions: The substantial reductions in RV/LV ratio and sPAP, short thrombectomy time, and improvements in functional outcome measures demonstrate that treating PE with Lightning 12 is safe and effective in a real-world population.