084 - Porto-hepatic Venous Shunt Resulting in Hepatic Encephalopathy Managed by Endovascular Embolization
Joe Khoury, DO/MBA – Resident, Interventional Radiology, Northwell Health; Asaph Levy, MD – Attending Physician, Interventional Radiology, Northwell Health; Jonathan Penner, MD – Resident, Interventional Radiology, Northwell Health; Jonathan Weinstein, MD – Attending Physician, Interventional Radiology, Northwell Health
Purpose: Intrahepatic portosystemic shunts are rare malformations between the portal and systemic circulations that can be congenital, spontaneous, or occur secondary to trauma, surgery, or long-standing portal hypertension. Although not always symptomatic, these shunts can occasionally present with hepatic encephalopathy. Endovascular embolization plays an important role in patients with symptomatic portosystemic shunts that are refractory to conservative management. Here, we highlight a case of a shunt that was managed by retrograde transcaval endovascular embolization.
Material and Methods: We present the case of a 65-year-old female with a history of NASH cirrhosis who presented to the hospital with altered mental status. On admission, her serum ammonia was 91, which was managed medically with rifaximin and lactulose and improved to 31. However, her altered mental status remained. A left portal vein to left hepatic vein shunt was identified on MRI. Interventional Radiology was consulted for endovascular embolization.
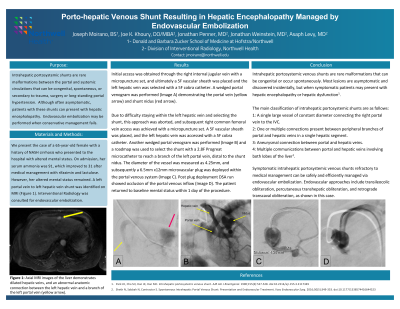
Results: Access was initially achieved through the right internal jugular vein, but a difficult take-off of the left hepatic vein into the IVC resulted in change of access to the right femoral vein. Re-access was achieved with a micro puncture set, and a 5F vascular sheath was placed and a 5F cobra catheter advanced into the IVC. A wedge portal venogram was performed, which allowed visualization of the origin of the left hepatic vein. Over a guidewire, the 5F cobra catheter was advanced into the left hepatic vein and multiple DSA runs performed. The fistulous connection was visualized and traversed using a 2.8 F Progreat microcatheter over a fathom wire. A 6.5 mm x 12 mm microvascular plug was deployed from the portal venous side. Post plug deployment DSA run showed occlusion of the portal venous inflow. Patient was back to baseline A&O x3 within 1 day of procedure.
Conclusions: Symptomatic intrahepatic portosystemic venous shunts refractory to medical management can be safely and efficiently managed via endovascular embolization. A variety of techniques have been described, including transileocolic obliteration, percutaneous transhepatic obliteration, and retrograde transcaval obliteration, as shown in this case.