042 - The Effect of Endovascular Therapy on Surgical Bypass in a Limb Preservation Practice
Richard Neville, MD – Associate Director, Department of Surgery, Inova Heart and Vascular Institute
Purpose: The options for management of infrainguinal peripheral arterial disease and limb revascularization has drastically changed in the last several decades. This has had a dramatic effect on the type of surgical bypass performed in a limb preservation program. Lower extremity bypass has been performed with autogenous vein as the preferred conduit. However, the complexity of bypasses has increased due to bypass after endovascular failure, lack of venous conduit, and poor distal arterial targets. We report this impact on bypass characteristics performed at a tertiary care center with an active limb preservation program.
Material and Methods: Patients undergoing infrainguinal surgical bypass from 2016 to 2022 performed by a surgeon associated with a limb preservation program were analyzed. The procedures were categorized based on bypass anatomy in regard to the outflow target artery (popliteal, anterior tibial/DP, posterior tibial/plantaris pedis, or peroneal). Bypasses were further analyzed based on conduit (vein, prosthetic) and anastomotic configuration—no adjunct, distal vein patch (DVP), anastomotic fistula, deep vein arterialization (DVA).
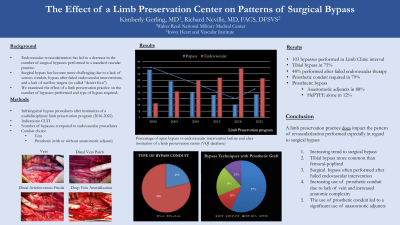
Results: A total of 103 surgical bypasses were performed over a 6 year period representing 28% of lower extremity revascularization procedures during that time. All bypasses were performed for symptoms of critical limb ischemia(rest pain, tissue loss). Vein bypass was performed in 22 patients (21.4%) with 20 tibial and 2 plantaris pedis bypasses. A prosthetic conduit (heparin bonded ePTFE) was used due to a lack of adequate vein, or in order to reach the appropriate distal target. ePTFE for tibial bypass was used in 59 patients (57%) with the following anastomotic configurations; 34 distal vein patch (33%), 7 distal arteriovenous fistula (6.8%), 7 prosthetic alone (6.8%), 11 deep vein arterialization (10.7%). In 22 patients (21.4%) prosthetic graft was used to bypass to the below knee popliteal level.
Conclusions: This bypass experience reflects a dramatic change in the type of bypass performed due to the continued development of endovascular procedures, especially below the knee. Tibial bypass is far more common than femoral-popliteal bypass with a concomitant shift towards the use of prosthetic conduit. This shift toward prosthetic graft utilization with anastomotic adjuncts now comprise the majority of bypasses performed for limb preservation. Mastery of these techniques will be important to continue to offer bypass to patients for healing and amputation prevention.