078 - Survival and Term-Outcomes of Open and Endovascular Surgical Repair of Unruptured Infrarenal Abdominal Aortic Aneurysms
Purpose: Endovascular Aortic Repair (EVAR) has become the standard management of Unruptured Infrarenal Abdominal Aortic Aneurysm (UIAAA); however, current evidence is limited and uncertain when compared to Open repair. Our study aimed to determine the survival, short and long-term outcomes of EVAR vs. Open in a Peruvian cohort of UIAAA.
Material and Methods: A single-center observational, analytical, longitudinal study using a retrospective registry of 251 patients treated (EVAR=205 vs. Open=46) for UIAAA during 2000-2017. Variables considered were baseline, comorbidities, clinical-surgical, type of treatment, short-term ( < 30 days) and long-term ( < 5 years) outcomes, postoperative mortality according to the Vascular Quality Initiative (VQI) Risk Score, survival curves including reoperation-free rate and according to size ( < 65 mm vs. >65 mm) of long-term UIAAA. All variables were grouped according to the treatment performed (EVAR vs. Open) and compared with descriptive, multivariate, Cox regression, and Kaplan-Meier survival statistical analyses.
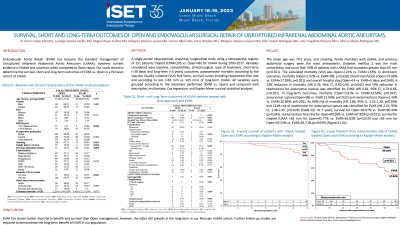
Results: The mean age was 74.5 years, and more than 50% of patients with UIAAA had diameters greater than 65 mm (p=0.021). The calculated mortality (VQI) was Open=2.21% vs. EVAR=1.65%. In short-term outcomes, mortality (Open=2.92% vs. EVAR=0%; p=0.039), blood transfusion (Open=72.68% vs. EVAR=17.39%; p=0.021) and overall hospital stay (Open=14 vs. EVAR=5 days; p=0.049). A 24% reduction in mortality (HR 0.76, 95% CI, 0.62-0.96, p=0.045) and 19% reduction in readmission for aneurysmal rupture was identified for EVAR (HR 0.81, 95% CI, 0.79-0.85, p=0.031). In long-term outcomes, mortality (Open=3.41% vs. EVAR=19.56%; p=0.047), aneurysmal rupture (Open=0% vs. EVAR 13.04%; p=0.032) and reinterventions (Open=2.43% vs. EVAR=10.86%; p=0.002). An 86% risk of mortality (HR 1.86, 95% CI, 1.32-2.38, p=0.039) and 121% risk of readmission for aneurysmal rupture was identified for EVAR (HR 2.21, 95% CI, 1.98-2.45, p=0.028). At 5 years, survival for Open=93.67% vs. EVAR=80.44% (p=0.043), reintervention free rate for Open=89.26% vs. EVAR=47.82% (p=0.021), survival for treated IUAAA < 65 mm for Open=95.77% vs. EVAR=63.63% (p=0.019) and >65 mm for Open=92.53% vs. EVAR=85.71% (p=0.059).
Conclusions: EVAR has shown better short-term benefit and survival than Open management; however, the latter still prevails in the long-term in our Peruvian UIAAA cohort. Further follow-up studies are required to demonstrate the long-term benefit of EVAR in our population.