071 - Effect of Amputation Type on Functional Status in Peripheral Arterial Disease: An Educational Review
Conner Reynolds, D.O. – Resident Physician, University of Arizona College of Medicine Tucson; Austin Shinagawa, M.D. – Resident Physician, Interventional Radiology, Kaiser Permanente Los Angeles; Geogy Vatakencherry, M.D. – Program Director, Vascular and Interventional Radiology, Kaiser Permanente Los Angeles
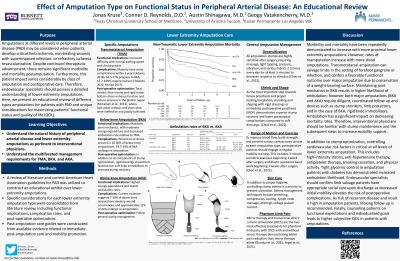
Purpose: Lower extremity peripheral arterial disease (PAD) is a growing cause of cardiovascular-related morbidity and mortality, affecting more than 230 million patients worldwide (Arday & Matsushita, 2021). Despite continued therapeutic advancement and vascular interventional radiologists' (VIR) growing role in limb ischemia, there remains significant morbidity and mortality postamputation. Furthermore, this patient impact varies considerably by type of amputation and postoperative care (Creager et al., 2021). Therefore, VIRs should possess a detailed understanding of lower extremity amputations. Here, we present an educational review of PAD amputations and unique considerations for maximizing patients’ functional status and quality of life (QOL).
Material and Methods: A review of literature and current American Heart Association guidelines for PAD was utilized to construct an educational exhibit over lower extremity amputations.
Results: In PAD, amputations at different levels (e.g. TMA, BKA, AKA) may be considered when patients develop critical limb ischemia, non-healing wounds with superimposed infection, or refractory ischemia revascularization (Narula et al., 2018, Busse et al., 2007). Morbidity and mortality have been repeatedly demonstrated to increase with more proximal lower extremity amputations (Cascini et al., 2020, Chopra et al., 2018). However, rates of reamputation increase with more distal amputations (Boyko et al., 2018). Transmetatarsal amputation can salvage limbs in the setting of forefoot gangrene or infection, and confers a favorable functional outcome over major amputation due to preservation of a weight-bearing surface (McCallum et al., 2012). Maintaining joint mechanics in BKA results in higher likelihood of ambulation; however both major amputations (BKA and AKA) require diligent, coordinated follow up and devices such as stump shrinkers, limb protectors, and in the case of BKA, knee immobilizers (Fergason et al., 2010).
Conclusions: Controlling cardiovascular risk factors is critical at all levels of lower extremity amputation. VIRs should confirm limb salvage patients have appropriate social care upon discharge as decreased initial mobility elevates the risk of post-operative complications (McCallum et al., 2012). Counseling patients on functional expectations and individualized goals leads to higher subjective QOL in patients with amputations (Creager et al., 2021).