079 - Removal of a TrapEase IVC Filter Using Dual "Kissing" Sheaths and Excimer Laser Assistance
Antanina Voit, MD – Vascular Surgery Physician Resident, Duke University Health System; Bryan Kozak, PA-C – Vascular Surgery Physician Assistant, Duke University Health System; Zachary Williams, MD – Assistant Professor of Surgery, Vascular and Endovascular Surgery, Duke University Health System
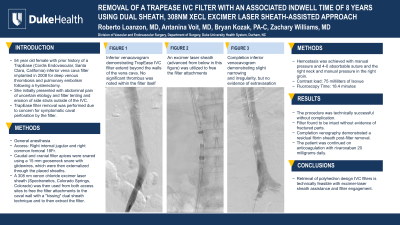
Purpose: A 54 year old female with prior history of a TrapEase (Cordis Endovascular, Santa Clara, California) inferior vena cava (IVC) filter implanted in 2008 for deep venous thrombosis and pulmonary embolism following a hysterectomy. She initially presented with abdominal pain of uncertain etiology and filter tenting and erosion of side struts outside of the IVC. TrapEase filter removal was performed due to concern for symptomatic caval perforation by the filter.
Material and Methods: The procedure was performed under general anesthesia. Right internal jugular and right common femoral 18 French sheaths were placed for access. Caudal and cranial filter apices were snared with guide wires, which were then externalized through the placed sheaths. A 308 nm xenon chloride excimer laser sheath (Spectranetics, Colorado Springs, Colorado) was then used both from jugular access and femoral access sites to free the filter attachments to the caval wall with a "kissing" dual sheath technique and to then extract the filter. A total of 75 milliliters of Isovue and 18.4 minutes of fluoroscopy time were required for procedure completion.
Results: The procedure was technically successful without complication. Completion venography demonstrated a residual fibrin sheath post-filter removal for which the patient was continued on anticoagulation with rivaroxaban 20 milligrams daily.
Conclusions: Retrieval of polyhedron design IVC filters is technically feasible with excimer-laser sheath assistance and appropriate filter engagement.