059 - Catheter Directed Thrombolysis in Setting of Pulmonary Embolism and Paradoxical Embolism
Justin Eichinger, Medical Student – Medical Student, University of Louisville School of Medicine; N Kemper, Medical Student – Medical Student, University of Louisville School of Medicine; Nana Ohene-Baah, MD – Attending Physician, Radiology, University of Louisville School of Medicine
Purpose: Paradoxical Embolism (PDE) is a serious form of thromboembolism often stemming from deep vein thrombosis that in combination with a patent foramen ovale (PFO) can introduce thromboemboli into the systemic circulation. Management of massive PDE can be accomplished using systemic or catheter-directed thrombolysis (CDT) using alteplase, or thrombectomy. Here we present a patient with bilateral PE and multiple arterial thromboembolisms who was successfully treated using CDT.
Material and Methods: This is a case study investigating the patient chart, imaging, and interventional radiology procedures performed in a single patient.
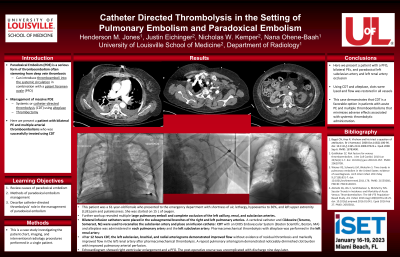
Results: This patient was a 61-year-old female who presented to the emergency department with shortness of air, lethargy, hypoexemia to 30%, and left upper extremity (LUE) pain and pulselessness. She was started on 15 L of oxygen. Upon further workup, the patient was found to have multiple large pulmonary emboli and complete occlusion of the left axillary, left renal, and left subclavian arteries.
Bilateral infusion catheters were placed in the subsegmental branches of the right and left pulmonary arteries. A vertebral catheter and Glidewire (Terumo, Somerset, NJ) were used to recanalize the subclavian artery and place an infusion catheter. CDT with alteplase was administered in each pulmonary artery and the left subclavian artery. Pharmacomechanical thrombolysis with alteplase was performed in the left renal artery.
After 12 hours CDT, the left subclavian, brachial, and radial arteriograms demonstrated improved flow without evidence of residual thrombosis and markedly improved flow in the left renal artery after pharmacomechanical thrombolysis. A repeat pulmonary arteriogram demonstrated noticeably diminished clot burden with improved pulmonary arterial perfusion.
Echocardiogram showed right ventricular enlargement and a PFO. The patient’s post operative course was uncomplicated and she was discharged nine days later.
Conclusions: Here we present a patient with a PFO, bilateral PEs, and paradoxical left subclavian artery and left renal artery occlusion. Using CDT with an EKOS Endovascular System (Boston Scientific, Boston, MA) and alteplase, clots were lysed and flow was restored in all vessels. This case demonstrates that CDT is a favorable option in patients with acute PE and multiple thromboembolisms that minimizes adverse effects associated with systemic thrombolytic administration.