142 - Contemporary Trends in Renal Artery Stenting for Renovascular Disease: Effect of Clinical Trials on Management
Edwin Takahashi, MD – Assistant Professor, Radiology, Mayo Clinic; Andrew Stockland, MD – Assistant Professor, Radiology, Mayo Clinic; Christopher Reisenauer, MD – Assistant Professor, Radiology, Mayo Clinic; Sanjay Misra, MD – Professor, Radiology, Mayo Clinic
Purpose: In the past two decades, randomized clinical trials regarding intervention for renal artery stenosis (RAS) were emerging. Among them are the STAR, ASTRAL, and CORAL trials. Additionally, the AHA, ACC, and AHRQ released statements regarding the interpretation of these trials’ findings, indicating that medical management alone is favorable over endovascular intervention. The impact of these trials on changes in the rates of intervention and outcomes is unknown. Thus, we investigated whether the conclusions may have influenced treatment modalities and outcomes of RAS.
Material and Methods: The National Inpatient Sample was queried between 2005 to 2019, for adult patients with RAS. Endovascular interventions included angioplasty and/or stenting. Cochrane-Armitage test was conducted to assess trends in proportion of endovascular intervention among those with RAS in three different time periods: 2005-2009 (pre-ASTRAL and -STAR), 2009-2014 (post-ASTRAL and -STAR) and 2014-2019 (post-CORAL). Multivariable logistic regression was used to assess patient profile of those who received endovascular intervention, non-routine discharge, and in-hospital mortality. Those with fibromuscular dysplasia and open intervention were excluded.
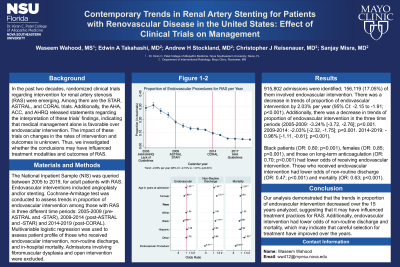
Results: 915,802 admissions were identified; 156,119 (17.05%) of them involved endovascular intervention. There was a decrease in trends of proportion of endovascular intervention by 2.03% per year (95% CI: -2.15 to -1.91; p< 0.001). Additionally, there was a decrease in trends of proportion of endovascular intervention in the three time periods (2005-2009: -3.24% [-3.72, -2.76]; p< 0.001. 2009-2014: -2.03% [-2.32, -1.75]; p< 0.001. 2014-2019: -0.96% [-1.11, -0.81]; p< 0.001). Black patients (OR: 0.80; p< 0.001), females (OR: 0.85; p< 0.001), and those on long-term anticoagulation (OR: 0.70; p< 0.001) had lower odds of receiving endovascular intervention. Those who received endovascular intervention had lower odds of non-routine discharge (OR: 0.47; p< 0.001) and mortality (OR: 0.63; p< 0.001).
Conclusions: Our analysis demonstrated that the trends in proportion of endovascular intervention decreased over the 15 years analyzed, suggesting that it may have influenced treatment practices for RAS. Additionally, endovascular intervention had lower odds of non-routine discharge and mortality, which may indicate that careful selection for treatment have improved over the years.