108 - Radiologic findings and endovascular management of lower GI bleed in a patient with celiacomesenteric trunk
Shashi Singh, MD – Director of Interventional Radiology, Interventional Radiology, Jacobi Medical Center
Purpose: Celiacomesenteric trunk (CMT) is a rare variant (0.5%) of the ventral branches of the abdominal aorta where the celiac trunk and superior mesenteric artery (SMA) have a common origin. It is usually asymptomatic, but may be discovered incidentally during imaging or surgical procedures. Anatomical variants of the celiac trunk have been thoroughly described in literature. Understanding these variants are important to surgeons and interventional radiologists to prevent vascular injury during procedures.
Material and Methods: We present a case of a 62-year-old woman with past medical history of diverticulosis s/p hemicolectomy in 2015 and arthritis managed with Plaquenil and prednisone who presented with acute onset hematochezia, abdominal cramping, and nausea. Patient appeared to be fatigued and found to be hypotensive with a blood pressure of 75/53 and anemic with a hemoglobin level of 7.1. 4 units of packed RBCs was administered. CT angiography of the abdomen and pelvis demonstrate moderately distended fluid filled bowel loops without evidence of active arterial bleeding. In addition, an uncommon vascular variant was identified of a combined celiac and mesenteric trunk. IR was consulted for angiogram and possible embolization of lower GI bleed.
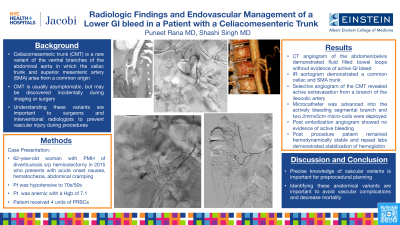
Results: Aortogram demonstrated a common celiac artery and SMA trunk known as a CMT. Selective angiogram of the CMT demonstrated active extravasation from a branch of the ileocolic artery. A microcatheter was advanced distally into the actively bleeding segmental branch of the ileocolic artery. Coil embolization was performed with two 2mm x 5cm endovascular coils. Post embolization angiogram did not show any further active extravasation of contrast. Post procedure, the patient was taken to the medical ICU and remained hemodynamically stable. Repeat labs demonstrated stabilization of hemoglobin. Colonoscopy was preformed and demonstrated no evidence of active bleeding. The patient as discharged on post procedure day 7 in stable condition.
Conclusions: The precise knowledge of vascular variants is very important for preoperative/preprocedural planning. Identifying and understanding these anatomic variants are important to avoid vascular complications and decrease morbidity.