050 - Assessing AI, Clinical Tools, and Biomarkers in Predicting Outcomes of Moderate to High-Risk Pulmonary Embolisms
Deepak Iyer, BS – Medical Student, George Washington University School of Medicine and Health Sciences; Subhash Gutti, BA – Medical Student, George Washington University School of Medicine and Health Sciences; Hannah Gissel, MD – Resident Physician, George Washington University Hospital; Bohan Liu, MD – Resident Physician, George Washington University Hospital; Daniel Scher, MD – Assistant Professor of Radiology, Interventional Radiology, George Washington University Hospital; Shawn Sarin, MD, MBA, FSIR – Assistant Professor of Radiology, Interventional Radiology, George Washington University Hospital
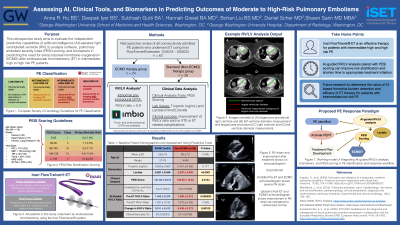
Purpose: To evaluate the independent predictive capabilities of artificial intelligence (AI)-assisted right ventricle/left ventricle (RV/LV) analysis software, pulmonary embolism severity index (PESI) scoring, and biomarkers in predicting the need for extracorporeal membrane oxygenation (ECMO) after endovascular thrombectomy (ET) in moderate to high-risk PE patients.
Material and Methods: PE patients who underwent ET using the Inari FlowTriever system between March 2018 and August 2022 were retrospectively reviewed. Baseline demographics, clinical history, procedural and clinical outcomes, relevant laboratory values, and post-ET ECMO use were recorded. Patients with available pre- and post-procedural chest CT pulmonary angiograms (CTPA) were further evaluated for RV/LV ratio calculation using Imbio’s RV/LV software. Clinical success was defined as an improvement in RV/LV ratio and no VTE or ET-related complications.
Results: Among PE patients treated with ET using the FlowTriever system included in this study (n=62), 38.7% (n=24; average age 56±16) of the patients required ECMO post-ET, while 61.3% did not (n=38; average age 60±13). Overall, clinical success was observed in 83.3% (20 of 24) of patients on ECMO and 97.4% (37 of 38) of patients not on ECMO. Patients who required ECMO were found to have significantly higher lactate levels (5.281±3.046 vs. 2.397±2.630, P< 0.0001) but not troponin levels (0.933±2.560 vs. 0.451±0.485, P=0.766). These patients also presented with higher PESI scores (125.26±35.10 vs. 102.51±25.33, P< 0.05). Pre- and post-ET CTPA were available for 54.2% (13 of 24) patients on ECMO and 50.0% (19 of 28) patients not on ECMO. Patients on ECMO experienced a greater change in pre- vs post-procedural RV/LV ratios (0.911±412 vs 0.430±0.273, P< 0.005). This difference was reflected in pre-procedural RV/LV ratios (1.942±0.376 vs. 1.480±0.312, P< 0.001), but not among post-procedural RV/LV ratios (1.031±0.193 vs. 1.072±0.226, P=0.383).
Conclusions: In our experience, ET using the Inari FlowTriever system is an effective therapy for moderate to high risk PE. Moreover, our study demonstrates that using AI-assisted RV/LV analysis paired with PESI scoring and lactate values can accurately predict the need for ECMO therapy following ET. Future work in improving PE risk stratification should thus include these metrics to assist in triage and optimize outcomes for high-risk VTE patients.