136 - Clinical Outcomes of Patients with Acute GI Tract Bleeding Treated with N-butyl-2-Cyanoacrylate Glue Embolization
Scott Nowakowski, MD – Director of Operations, Vascular and Interventional Radiology, Icahn School of Medicine at Mount Sinai; Vivian Bishay, MD – Assistant Professor of Radiology, Vascular and Interventional Radiology, Icahn School of Medicine at Mount Sinai; Kirema Garcia-Reyes, MD – Assistant Professor of Radiology, Vascular and Interventional Radiology, Icahn School of Medicine at Mount Sinai; Rahul Patel, MD – Assistant Professor of Radiology and Surgery, Vascular and Interventional Radiology, Icahn School of Medicine at Mount Sinai; Dan Shilo, MD – Assistant Professor of Radiology, Vascular and Interventional Radiology, Icahn School of Medicine at Mount Sinai; Edward Kim, MD – Assistant Professor of Radiology and Surgery, Vascular and Interventional Radiology, Icahn School of Medicine at Mount Sinai; Robert Lookstein, MD MHCDL FSIR FAHA FSVM – Professor of Radiology and Surgery, Executive Vice Chairman, Vascular and Interventional Radiology, Icahn School of Medicine at Mount Sinai; Aaron Fischman, MD FSIR FCIRSE FSVM – Professor of Radiology, Urology and Surgery, Vascular and Interventional Radiology, Icahn School of Medicine at Mount Sinai
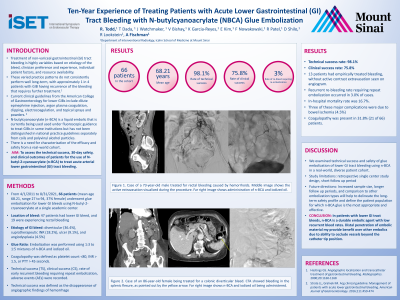
Purpose: To assess clinical outcomes of patients with acute arterial gastrointestinal (GI) tract bleeding treated with N-butyl-2-cyanoacrylate (NBCA).
Material and Methods: We reviewed procedural and clinical information in 106 patients who underwent GI embolization between September 2016 and June 2019 at a single center. Embolization with exclusively NBCA was performed in 41 patients (17 female, mean age 67.8 years) with acute upper GI (n = 22), lower GI (n = 17), rectal (n=2) bleeding. The most common etiology of bleed was diverticular (n=9), ulcer (n=7), angiodysplasia (n=7), and GI anastomosis (n=4). Embolization was performed using 1:3 to 1:5 mixtures of NBCA and iodized oil. Four patients had empirically treated bleeding, without active contrast see on angiogram. Coagulopathy (defined as platelet count < 80, INR >1.5, or PTT >45 seconds) was present in 39% (16/41) of patients. Technical success (defined as the disappearance of angiographic findings of hemorrhage on completion), early recurrent bleeding (defined as clinical signs of re-bleeding requiring medical, radiologic, endoscopic, or surgical treatment at the treated focus within 30 days of embolization) and complications, were recorded.
Results: The technical success rate was 97.5%. In one case there was persistent contrast extravasation after embolization of a third order branch of the right colic artery, thought to be likely arising from collateral, that was unable to be accessed from a retrograde approach. Early recurrent re-bleeding occurred in 4 patients (9.7%), of which two patients had empirically treated bleeds. Three patients (7.3%) presented with clinical signs/symptoms of bowel ischemia post-procedurally; two patients had complete resolution with medical management, and one patient had bowel ischemia complicated by intestinal perforation. Surgical management was recommended, but patient declined.
Conclusions: Findings in this large cohort adds to the growing body of evidence that NBCA is a durable agent for GI tract bleeds with low recurrent bleed rates despite coagulopathy. Distal penetration of embolic material may provide benefit over other embolics due to ability to occlude vessels beyond the catheter tip position.