Colleen Corrado, BS – Medical Student, The George Washington University School of Medicine & Health Sciences; Anna Hu, BS – Medical Student, The George Washington University School of Medicine & Health Sciences; Subhash Gutti, BA – Medical Student, The George Washington University School of Medicine & Health Sciences; Bohan Liu, MD – Resident Physician, Department of Radiology, The George Washington University Hospital; Hannah Gissel, MD – Resident Physician, Department of Radiology, The George Washington University Hospital; Shawn Sarin, MD – Associate Professor, Department of Radiology, The George Washington University Hospital; Daniel Scher, MD – Assistant Professor, Department of Radiology, The George Washington University Hospital
Purpose: Pelvic Venous Insufficiency (PVI) is a common source of chronic pelvic pain impacting women globally. The symptoms of PVI are often non-specific and may overlap with other pathologies resulting in underdiagnosis and lack of treatment. The purpose of this study is to provide an overview of the current literature on PVI.
Material and Methods: A review of the literature was performed using PubMed.
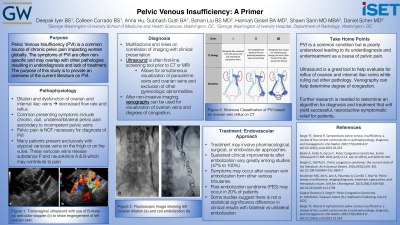
Results: The pathophysiology of PVI involves dilation and dysfunction of the ovarian and internal iliac veins, resulting in decreased flow rate and reflux. Common presenting symptoms include chronic, dull, unilateral/bilateral pelvic pain secondary to incompetent pelvic veins; however, pelvic pain is not necessary for diagnosis. Many patients exclusively present with varicose veins on the thigh, and up to 40% of patients may also have vulvar varicose veins. Varicose veins release neurotransmitters, such as substance P and neurokinins A and B, which may contribute to pain.
The diagnosis of PVI is multifactorial and relies on the correlation of imaging with clinical presentation. Ultrasound is the first-line screening tool prior to CT or MRI of the pelvis. These imaging modalities allow for simultaneous visualization of the parauterine veins and ovarian veins and exclusion of other gynecologic abnormalities. The gold standard following non-invasive imaging techniques is venography allowing for visualization of the diameter of the ovarian veins and their degrees of congestion.
Treatment of PVI may involve a pharmacologic, surgical, or endovascular approach. A lack of data surrounding treatment options results in the absence of a universally standard protocol. Sustained clinical improvements after embolization vary greatly among studies from 47% to 100%. Symptoms may reoccur after ovarian vein embolization from other tributaries in the venous network. Postembolization syndrome may occur in 20% of patients. Some studies suggest that there is not a statistically significant difference in clinical results with bilateral vs. unilateral embolization.The complications associated with a percutaneous embolization include symptom recurrence and non-target embolization.
Conclusions: While PVI is a common condition, poor knowledge of the condition and ambiguity of symptoms leads to underdiagnosis and subsequent lack of treatment. Further research is necessary to determine an algorithm for diagnosis and treatment that will yield successful, reproducible symptomatic relief for patients.