041 - IR vs OR: Chest Port Insertion outcomes and complications
Micahel McGarry, MD – Head, Interventional Radiology, Mercy Catholic Medical Center
Purpose: Implanted chest port is the gold standard for chemotherapy and immunotherapy delivery. Successful implantation requires technical expertise and availability of surgery and interventional radiology teams. The purpose of this study is to identify technical characteristics and complications between IR and OR implanted ports.
Material and Methods: A retrospective, single-institution EMR review was done identifying exam and CPT codes associated with port insertion, revision and removal performed in the Interventional Radiology suite and operating room between January 2017 and October 2020. Demographic indicators included age and gender, as well as type of cancer and immunologic disease. Venous access type, laterality and final positioning of catheter tip were reviewed from intraprocedural image records available in PACS. Fluoroscopy time, catheter duration, immediate and late complications were also evaluated.
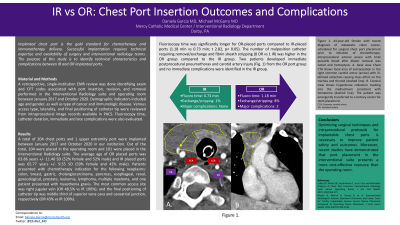
Results: A total of 204 chest ports and 1 upper extremity port were implanted during January 2017 and October 2020 in our institution. Out the total, 104 were placed in the operating room and 101 were placed in the Interventional Radiology suite. The average age of O.R placed ports was 63.86 years +/- 11.40 SD (52% female and 52% male) and IR placed ports was 65.77 years +/- 9.55 SD (59% female and 42% male). Patients presented with chemotherapy indication for the following neoplasms: colon, breast, gastric, cholangiocarcinoma, pancreas, esophageal, renal, gynecological, prostate, leukemia, lymphoma, multiple myeloma and one patient presented with myasthenia gravis. The most common access site was right jugular vein (OR 48,5% vs IR 100%); and the final positioning of catheter tip was middle third of superior vena cava and cavoatrial junction, respectively (OR 43% vs IR 100%). Fluoroscopy time was significantly longer for OR placed ports compared to IR placed ports (1.18 min vs 0.73 min; t 2.82, p< 0.05). The number of malpositioned catheter requiring removal/exchange and fibrin sheath stripping (8 OR vs 1 IR) was higher in the OR group compared to the IR group. Two patients developed immediate postprocedural pneumothorax and carotid artery dissection from the OR port group and no immediate complications were identified in the IR group.
Conclusions: Optimization of implantable port insertion techniques and protocol, considering technical expertise and supplies/infrastructure value in the hospital setting is necessary to improve patient’s outcomes and decrease healthcare cost.