076 - Prone Positioning for Expedient Angioembolization Following Renal Mass Biopsy
Amir Noor, MD – Clinical Assistant Professor, Vascular and Interventional Radiology, New York University School of Medicine
Purpose: Rarely, the Interventional Radiologist may need to perform both percutaneous biopsy and embolization of a renal mass. Particularly for hypervascular lesions, this request poses a unique challenge given the associated high risk of hemorrhage following biopsy. If biopsy is performed first, then the patient must subsequently be positioned supine, prepped and draped, arterial access obtained, and the appropriate renal artery branch selected. This time-consuming process may predispose to greater risk of hemorrhage before successful embolization is achieved. If instead angioembolization is performed prior to biopsy, then pathologic analysis may be hindered by presence of embolic material. We describe the usage of radial access in prone position to address both issues.
Material and Methods: A 30 year-old-woman was referred for management of an incidentally found left renal angiomyolipoma. She was undergoing workup for tuberous sclerosis, but did not have an established diagnosis. Given the patient’s significant anxiety surrounding her diagnosis and recent 10lb unintentional weight loss over the course of 4 months, decision was made to also perform confirmatory biopsy of the left renal angiomyolipoma.
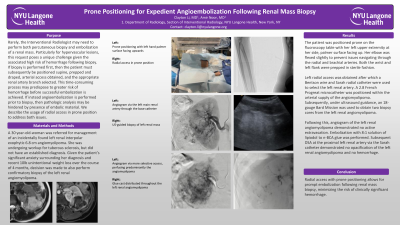
Results: The patient was positioned prone on the fluoroscopy table with her left upper extremity at her side, palmer surface facing up. Her elbow was flexed slightly to prevent issues navigating through the radial and brachial arteries. Both the wrist and left flank were prepped in sterile fashion.
Left radial access was obtained after which a Bentson wire and Sarah radial catheter were used to select the left renal artery. A 2.8 French Progreat microcatheter was positioned within the arterial supply of the angiomyolipoma. Subsequently, under ultrasound guidance, a 18-gauge Bard Mission was used to obtain two biopsy cores from the left renal angiomyolipoma.
Following this, angiogram of the left renal angiomyolipoma demonstrated no active extravasation. Embolization with 8:1 solution of lipiodol to n-BCA glue was performed. Subsequent DSA at the proximal left renal artery via the Sarah catheter demonstrated no opacification of the left renal angiomyolipoma and no hemorrhage.
Conclusions: Radial access with prone positioning allows for prompt embolization following renal mass biopsy, minimizing the risk of clinically significant hemorrhage.