037 - Mechanical thrombectomy to support creation or revision of TIPS/DIPS in patients with portal/mesenteric vein thrombus.
Zeeshan Toor, MD – Radiology Resident, NYP - Columbia University Irving Medical Center; Christopher Harnain, MD – Interventional Radiologist, Cornell University Medical Center; Noor Ahmad, MD – Interventional Radiologist, Columbia University Irving Medical Center
Purpose: To assess the safety and effectiveness of the Indigo System for mechanical thrombectomy supporting the creation and revision of transjugular and direct intrahepatic portosystemic shunts (TIPS and DIPS) in patients with portal and/or mesenteric vein thrombus.
Material and Methods: This was a single-center retrospective review of patients who underwent mechanical thrombectomy of portal and/or mesenteric vein thrombus with Indigo to support TIPS or DIPS creation or revision at our institution between October 2016 and November 2021. If indicated, venoplasty or stent placement were also performed. We assessed procedural, clinical, and safety outcomes.
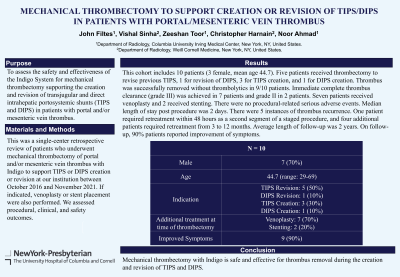
Results: This cohort includes 10 patients (3 female, mean age 44.7). Five patients received thrombectomy to revise previous TIPS, 1 for revision of DIPS, 3 for TIPS creation, and 1 for DIPS creation. Thrombus was successfully removed without thrombolytics in 9/10 patients. Immediate complete thrombus clearance (grade III) was achieved in 7 patients and grade II in 2 patients. Seven patients received venoplasty and 2 received stenting. There were no procedural-related serious adverse events. Median length of stay post procedure was 2 days. There were 5 instances of thrombus recurrence. One patient required retreatment within 48 hours as a second segment of a staged procedure, and four additional patients required retreatment from 3 to 12 months. Average length of follow-up was 2 years. On follow-up, 90% patients reported improvement of symptoms.
Conclusions: Mechanical thrombectomy with Indigo is safe and effective for thrombus removal during the creation and revision of TIPS and DIPS.