086 - Impact of Anatomical Location in the Outcomes Following Endovascular Repair of Abdominal Aortic Aneurysms
Roshan Panda, BS – Medical Student, University of Nevada, Reno School of Medicine; Shawn Thomas, MPH – PhD Candidate, University of Nevada, Reno School of Public Health
Purpose: The current approach to abdominal aneurysm (AAA) repair uses anatomical location during management and approach to surgery. However, there is limited data on the impact of AAA location on the outcomes after surgical repair. Our study evaluates how proximal and distal extent variations in anatomical location affects 30-day mortality and the major adverse events for endovascular AAA repair.
Material and Methods: Data was collected from the Targeted Vascular Procedure files from American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) between 2016 to 2020. All patients undergoing endovascular repair for an abdominal aortic aneurysm with information on proximal and distal extent (n = 8003) were included in the analysis. The prevalence of those who died and differences in major adverse events for proximal and distant extents were calculated. Logistic regression was used to calculate associations between proximal and distal extents and 30-day mortality, while adjusting for the effects of gender, age, elective surgery, history of congestive heart failure, ASA category, bleeding disorder, and BMI.
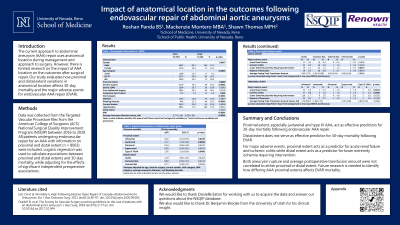
Results: Of 8003 patients who underwent endovascular surgery, 186 (2.3%) died. Proximal, but not distal, extent, was a statistically significant predictor of 30-day mortality. Patients receiving juxtarenal repair were more likely to die within 30 days compared to those receiving repair in another location [adjusted Odds Ratio (aOR)=2.27, 95% confidence interval (CI)=1.29-3.99, p=0.0043]. Patients receiving Type IV TAAA repair were more likely to die within 30 days compared to those receiving repair in another location (aOR=2.95, 95% CI=1.01-8.68, p=0.0490).
Conclusions: Proximal extent, especially juxtarenal and type IV AAA, act as effective predictors for 30-day mortality following endovascular AAA repair. For major adverse events, proximal extent acts as a predictor for acute renal failure and ischemic colitis while distal extent acts as a predictor for lower extremity ischemia requiring intervention.