135 - Malignancy Associated Superior Vena Cava Syndrome
Chadi Diab, MD – Assistant Professor, University of Kentucky
Purpose: Superior vena cava (SVC) syndrome occurs due to obstruction of the SVC. Symptoms include facial/neck and upper extremity swelling, shortness of breath, cough, airway compromise, syncope, dizziness, or coma. An estimated 15,000 cases of SVC syndrome occur annually in the USA with an incidence of 1/650-3100. Causes include mediastinal malignancy, fibrosing mediastinitis, and thrombosis due to pacemaker leads or central venous catheter. This case highlights the treatment of a patient with malignancy associated SVC syndrome.
Material and Methods: Patient is a 52yo F with PMH of stage IV NSCLC s/p right upper lobectomy. She presented with 2-3 days of neck/face swelling, chest pain, shortness of breath, cough, and left arm pain/numbness. CTV showed occlusion of the SVC, bilateral subclavian, and bilateral IJ veins; scattered groundglass opacities; bilateral pulmonary nodules and osseous metastases were unchanged. IR recommended venogram with thrombectomy for treatment of SVC syndrome.
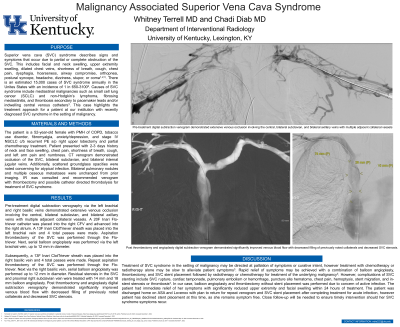
Results: Initial venogram via the left brachial and right basilic veins showed occlusion of the central, bilateral subclavian, and bilateral axillary veins with adjacent collaterals. A 20F Inari Flo-triever was placed into the right CFV. A 13F Inari ClotTriever was placed in the left brachial vein and 4 passes were made. Aspiration thrombectomy of the SVC was performed through the Flo-triever. Serial balloon angioplasty was performed up to 12 mm. This process was repeated via the right basilic vein. Residual stenosis in the SVC and right subclavian vein were dilated with 14 mm and 18 mm balloons. Repeat venogram showed improved flow with decreased filling of collaterals and improved SVC stenosis.
Conclusions: Treatment of SVC syndrome with chemotherapy/radiotherapy may be slow to alleviate symptoms. Rapid symptom relief may be achieved with balloon angioplasty, thrombectomy, and/or SVC stenting. Complications of SVC stenting include rupture, cardiac tamponade, PE or hemorrhage, hematoma, stent migration, and in-stent stenosis/thrombosis. In our case, angioplasty and thrombectomy without stent placement was performed due to concern of active infection. She had immediate relief of her symptoms. She was discharged home on ASA and Lovenox with plan to return for SVC stent placement after completing treatment for acute infection, however she declined stent placement as she remains symptom free. Close follow-up will be needed to ensure timely intervention should her SVC syndrome recur.