026 - Role of Interventional Radiology in the Management of Cervical Ectopic Pregnancies
Mihir Patel, MD – Assistant Professor, Diagnostic and Interventional Imaging, McGovern Medical School at UTHealth; Christopher Latour, BS, MBA – Medical Student, McGovern Medical School at UTHealth; Alexa Levey, MD – Assistant Professor, Diagnostic and Interventional Imaging, McGovern Medical School at UTHealth
Purpose: Cervical ectopic pregnancies are rare and there is currently no standard management for these complex cases as dilation and curettage (D&C) alone could cause excessive bleeding. Uterine artery embolization (UAE) is employed to control bleeding in these high-risk cases. Here we discuss two cases of cervical ectopic pregnancies that were successfully treated with UAE prior to D&C.
Material and Methods: The principle steps for UAE are similar for both procedures. The arterial system was accessed via the common femoral artery. An aortogram was performed to assess for collateral supply from ovarian arteries. Catheters were positioned in the horizontal segment of the uterine artery proximal to the cervicovaginal branch. Gelfoam and Embosphere microspheres were utilized for embolization for the first and second case, respectively.
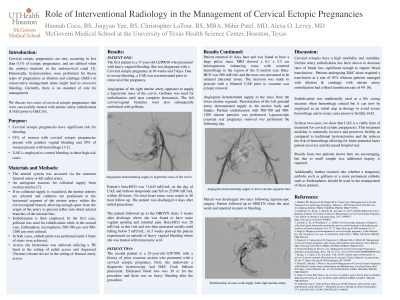
Results: The first patient is a 37 y.o. G2P0010 who presented with a cervical ectopic pregnancy. Due to severe bleeding, a UAE was recommended prior to removal of the pregnancy. Embolization was performed with Gelfoam. The patient underwent balloon tamponade of the cervical ectopic pregnancy the same day. No fetal heart tones were noted at 48 hour follow up and the patient was discharged 4 days after initial procedures. At a 3 week follow up the patient had vaginal spotting and minimal pain. The second patient is a 25 y.o. G2P1001 with a prior cesarean section who presented with a cervical ectopic pregnancy. She was treated with D&C with a Cook balloon placement. The patient returned with a pelvic mass presumed to be retained placental tissue. A bilateral UAE was planned due to the mass being highly vascular. The uterine arteries were catheterized and particle embolization was performed. The patient was discharged two days following laparoscopic surgery. She followed up to OBGYN clinic the next week with no pain or bleeding.
Conclusions: UAE has been shown to decrease rates of blood loss significant enough to require blood transfusions. Patients undergoing D&C alone required a transfusion at a rate of 30% whereas patients managed with D&C and UAE had a blood transfusion rate of 4%. In these two cases, we show that UAE is a viable form of treatment for cervical ectopic pregnancies. This treatment modality is minimally invasive and preserves fertility compared to traditional hysterectomies and the reduces the risk of hemorrhage allowing for potentially faster patient recovery and shorter hospital stay.