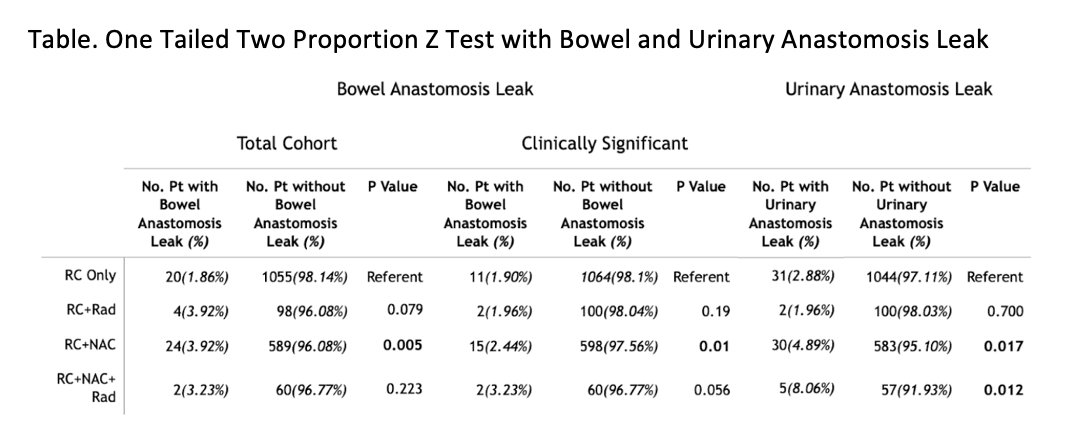
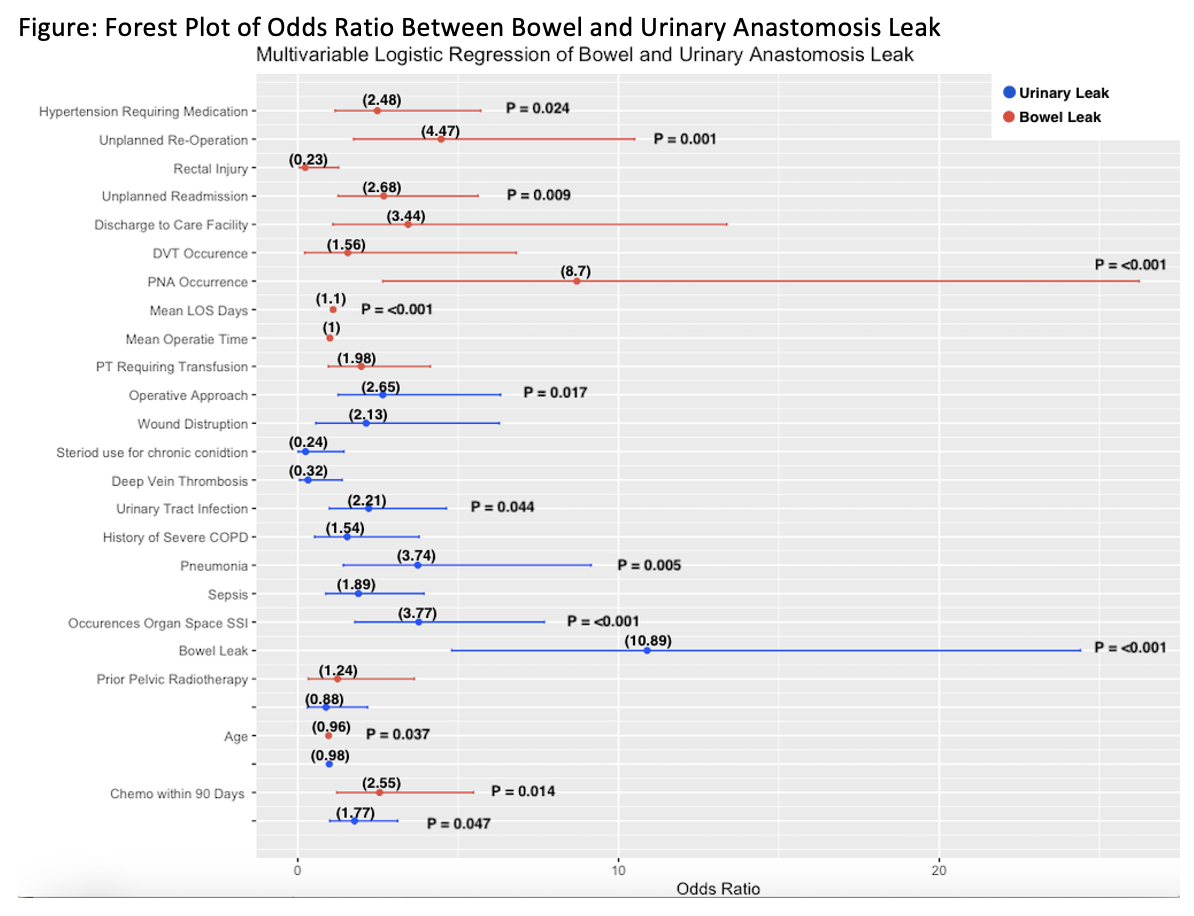
Introduction: Neoadjuvant chemotherapy (NAC) and radical cystectomy (RC) is the standard of care for MIBC. A previous study showed that prior pelvic radiation (RAD) was not associated with diversion related complications, however the effects of NAC have not been discussed in literature. The objective of this analysis is to determine if correlations exist between prior pelvic radiation and/or NAC before RC and urinary tract anastomotic leak following RC. Methods: The 2019 and 2020 NSQIP data was analyzed for cystectomy patients. Patient that met the inclusion criteria of pathological stage of MIBC (pT Stage = T2, T2a, T2b, T3, T3a, T3b, T4, T4a, T4b) were included. Patients were divided into 4 groups: RC only, NAC+RC, RAD+RC, RAD+NAC+RC. Then patients were subgrouped to those that had bowel and urinary anastomosis failure. Clinically significant bowel anastomosis leak was defined when intervention was performed (interventional radiological or reoperation). Results: A total of 1852 patients met the inclusion criteria. Among the cohort, 1075 (58%) Patients were treated with RC alone, 102 (5.5%) patients received prior pelvic radiation, 613 (33%) received chemotherapy, and 62 (3.3%) patients received both chemotherapy and pelvic radiation prior to RC. Overall, bowel anastomosis failure was 2.7% and urinary anastomosis failure rate was 3.7%. The RC+NAC group had increased clinically significant bowel (p=0.01) and urinary anastomosis (p=0.02) failure compared to the RC only group. The RC+NAC+RAD had no significance increase in bowel anastomosis failure (p=0.06) but was seen to have higher rate of urinary leak (p=0.01) (Table). Independent variables associated with bowel and urinary anastomotic failure included NAC in both regressions (Figure). Conclusions: We conclude that there is an increased rate of bowel and urinary anastomotic leak in the NAC+RC group and increased urinary anastomotic leak RC+NAC+RAD group compared RC only group. SOURCE OF Funding: n/a