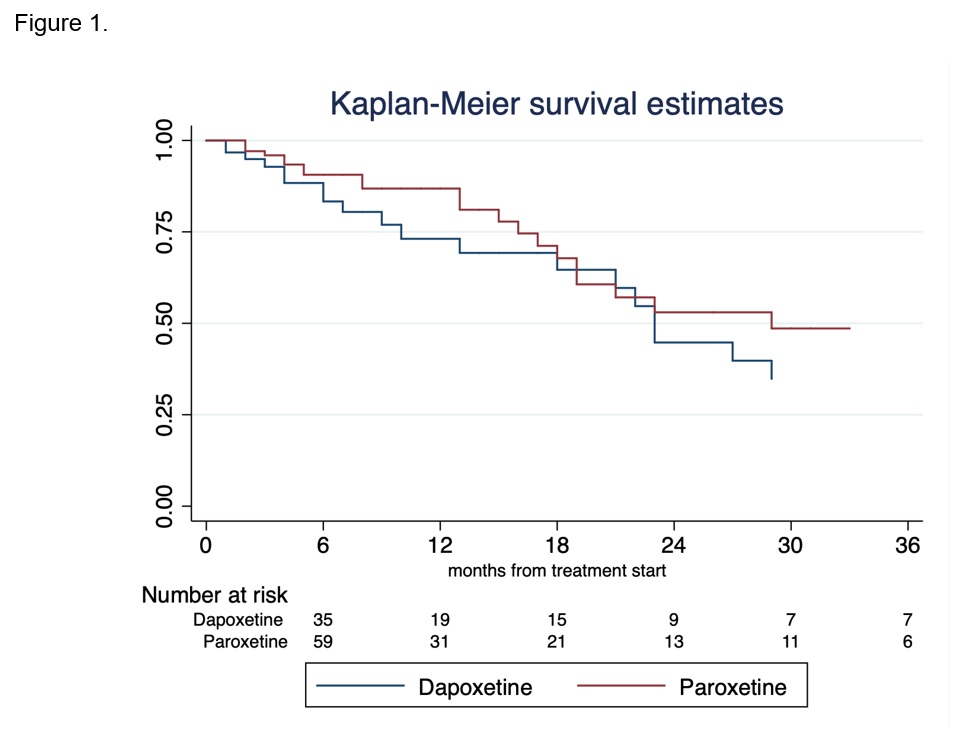
Introduction: Oral therapy for premature ejaculation (PE) has been associated with high drop-out rates due to side effects and poor results. We compared patients compliance to dapoxetine prn vs. paroxetine OaD in men with PE in a real-life setting. Methods: Data from 4105 patients with sexual dysfunctions prospectively collected at a single Sexual Medicine clinic in 2005-2022 were analysed. Overall, 342(8.3%) patients complained of PE and were treated either with dapoxetine 30-60mg prn or paroxetine 20mg OaD according to patients’ profile and preference. All completed the Premature Ejaculation Diagnostic Tool (PEDT) and the IIEF before and over the treatment course. Patients were re-assessed at 3 months from treatment start and thereafter every 6 months or as needed. Kaplan-Meier estimated treatment drop-out rates over time. Cox regression analysis assessed predictors of treatment discontinuation. Results: Median (IQR) age was 47(36, 61) years. Median baseline PEDT score was 15 (10,17.5). Of all, 151(44%) and 191(56%) patients were treated with dapoxetine and paroxetine respectively. Patients receiving dapoxetine were younger (40(30,48) vs. 56(41,67);p < 0.0001) and depicted worse baseline PEDT (16(14,18) vs. 8(3,14);p < 0.0001) as compared with those receiving paroxetine. Overall, 329(96%) discontinued the drugs at some point throughout the treatment course, showing only a slight mean improvement of PEDT from baseline of -0.4(95%CI:-0.8,1.7) and -0.8(95%CI:-0.7,1.3) with dapoxetine and paroxetine, respectively. At Kaplan-Meier (Figure-1) the two groups did not differ in terms of treatment dropout over time (p=0.3), with estimated discontinuation rates of 27%(15,45) and 55%(37,75) at 12 and 24 months for dapoxetine and 13%(7,24) and 47%(32,65) for paroxetine. Younger patients were at higher risk of treatment drop-out (HR:0.95,95%CI:0.91,0.99;p=0.03) after accounting for PEDT, IIEF-EF and type of treatment. Conclusions: PE still represents a therapeutic challenge with high treatment drop-out rates and only minor improvements. Younger patients appear at higher risk of oral therapies discontinuation and maybe better candidates for a multimodal treatment. SOURCE OF Funding: None