Resident Physician University of Wisconsin School of Medicine and Public Health
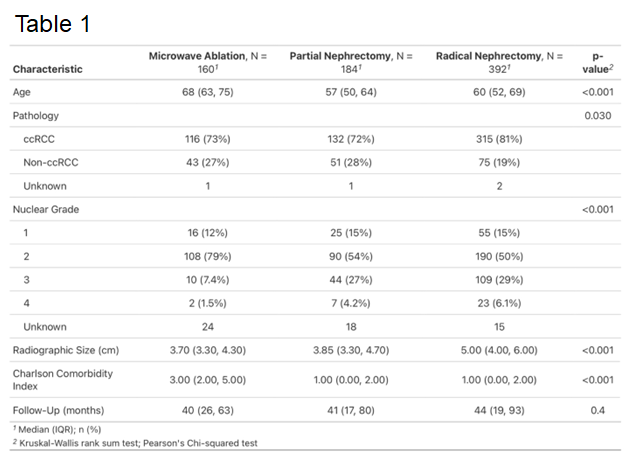
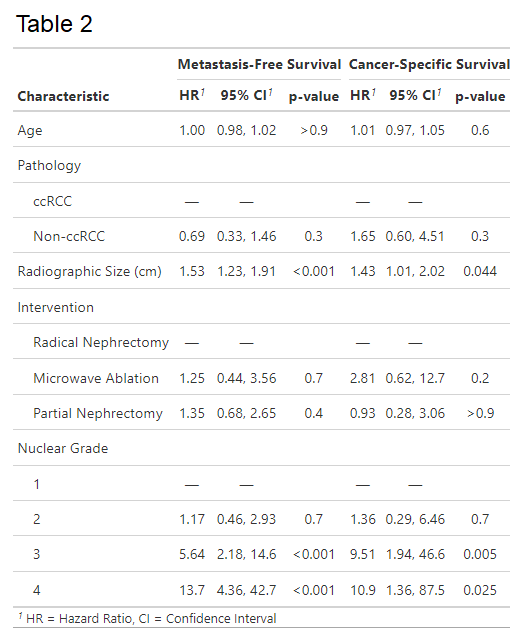
Introduction: Current AUA guidelines recommend radiofrequency ablation (RFA) or cryoablation be considered only for renal masses < 3 cm. However, microwave ablation (MWA) reliably generates larger ablation zones compared to other ablation modalities. This study compared oncologic outcomes between surgery and MWA in patients with renal masses between 3 and 7 cm. Methods: Data was analyzed for consecutive patients with 3 to 7 cm renal cell carcinoma (RCC) treated with MWA, radical nephrectomy (RN), or partial nephrectomy (PN), excluding patients with metastases or tumor thrombus. Local recurrence-free, metastasis-free, and cancer-specific survival were estimated using Kaplan-Meier method. Variables associated with survival were determined using Cox proportional hazard models. Results: Of 732 patients, 160 (22%) underwent MWA, 184 (25%) underwent PN, and 392 (53%) underwent RN (Table 1). Patients treated with MWA were older and more comorbid (p < 0.001). Patients who underwent RN had larger tumors (p < 0.001) and higher nuclear grade (p < 0.001). Median follow-up was 40, 41, and 44 months following MWA, PN, and RN (p=0.4). 5-year local recurrence free survival was lower for MWA (86%) compared to PN (98%) and RN (98%) (p < 0.0001). No differences were noted in metastasis-free or cancer-specific survival between the three cohorts (p=0.13 and p=0.85). Adjusting for age, pathology, radiologic size, and nuclear grade, MWA was associated with similar metastasis-free and cancer-specific survival compared to surgery (Table 2). Of 18 patients with local recurrence following MWA (11%), 13 underwent repeat ablation, 3 pursued surveillance, 1 had stereotactic radiation, and 1 underwent nephrectomy. After 2nd ablation, 12/13 (92%) patients had no recurrence of disease at median 19 months. Conclusions: Microwave ablation for 3 to 7 cm renal cell cancer has higher rates of local recurrence, which may be salvaged by repeat treatment. There was no difference in metastatic progression or cancer specific survival compared to surgery. SOURCE OF Funding: N/A