Resident Physician University of Wisconsin School of Medicine and Public Health
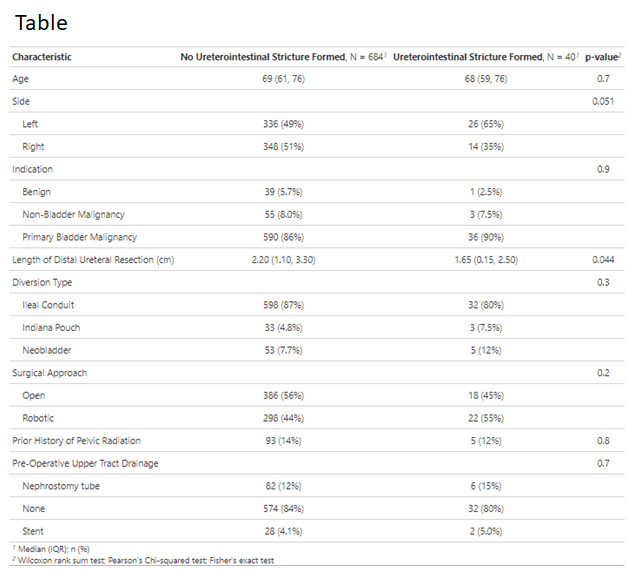
Introduction: Benign ureterointestinal anastomotic (UIA) strictures are a morbid complication following cystectomy with urinary diversion. Data from renal transplantation literature suggests that shorter ureters may result in fewer anastomotic strictures due to improved vascularization of the re-implanted segment. We evaluated whether length of distal ureteral resection may impact rates of UIA strictures in cystectomy patients. Methods: A database of patients who underwent cystectomy with urinary diversion from 2015 to 2022 was analyzed. All cases were performed by a single surgeon to control for variations in surgical technique. Distal ureteral resections were routinely sent for final pathology. Length of this resection was collected from pathology reports. Benign UIA strictures were confirmed with renal scintigraphy, antegrade nephrostogram, or endoscopic evaluation. Relationship between stricture formation and clinical parameters were assessed using T-tests, Chi-squared tests, and multivariable analysis. Results: A total of 362 patients underwent cystectomy with urinary diversion from 2015 to 2022. Of the cohort, 35 (9.6%) patients developed UIA strictures. Median time to stricture formation was 12.5 months (IQR 4-30). Of the 724 ureteral anastomoses among the 362 patients, 40 anastomoses developed benign strictures (6%). Median distal ureteral length resected was significantly longer among anastomosis that did not form a stricture (2.2 cm vs 1.65 cm, p=0.044, Table). Strictures more commonly formed on the left side, although this did not reach significance (65% vs 35%, p=0.051). Multivariable logistic regression adjusting for surgical approach, prior radiation, ureteral side, and urinary diversion type demonstrated longer distal ureteral resections were associated with a significantly lower risk of ipsilateral stricture formation (OR 0.74, 95% CI 0.58-0.94). Conclusions: The etiology of benign UIA strictures is multifactorial. Vascular compromise is a critical hypothesis. We found that longer distal ureteral resections (and thus shorter ureters) were associated with a significantly lower risk of stricture formation in cystectomy patients, consistent with renal transplantation data. SOURCE OF Funding: N/A