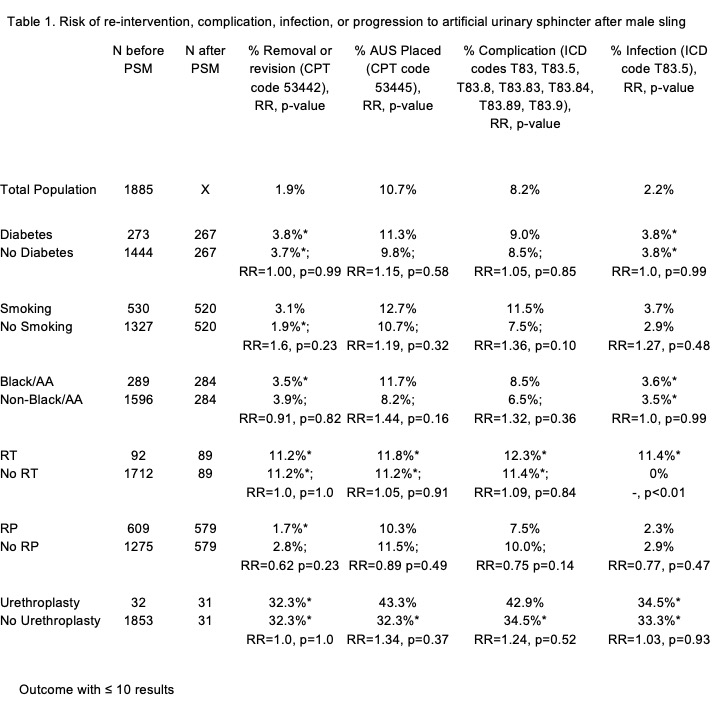
Introduction: Male slings (MS) are treatment for stress urinary incontinence, with an incomplete understanding of which patients may have treatment failure or undergo treatment progression to artificial urinary sphincter (AUS) placement. Current studies come from high volume centers, which raises concerns regarding the generalizability to lower volume urologists. Therefore, we sought to leverage a multi-national database to further understand which patient characteristics are associated with risk for device failure or complications to provide “real-world” outcomes and help guide patient counseling. Methods: We queried the TriNetX database for all adult patients undergoing MS. We evaluated the impact of age, body mass index, race, ethnicity, diabetes (DM), smoking history, history of radiation therapy (RT), history of radical prostatectomy (RP) and history of urethroplasty on select clinical outcomes following MS placement (CPT 53440). We assessed the rate of sling revision/removal (CPT 53442), progression to AUS placement (53445), rate of complication (ICD codes T83, T83.5, T83.8, T83.83, T83.84, T83.89, T83.9), and rate of infection (ICD T83.5). Analytics were performed on TriNetX which calculated risk ratios (RR). We evaluated our outcomes first on the entire population and then repeated analyses for each individual comparison cohort using the remaining demographic variables to perform propensity score matching (PSM). Notably, outcomes with less than 10 results are truncated in the TriNetX database to protect anonymity and avoid thin data. Results: Analyses were run on September 22nd, 2022. Approximately 2% and 10% of MS patients have their implant removed/revised or progress to AUS, respectively (Table 1). Overall complication rates were 8.2% and risk for infection 2.2%. Only a history of RT was associated with an increased risk of infection (11.4% vs 0%, p<0.01). No other PSM comparisons (race/ethnicity, DM, smoking history, RP, and urethroplasty) demonstrated statistical significance. Conclusions: Few patients go on to have removal or AUS placement following MS. Radiation may have an association with increased infection risk but interpretation of our results is limited based on rounding inherent to the data source. Repeat analyses with larger sample sizes may verify our results. SOURCE OF Funding: none