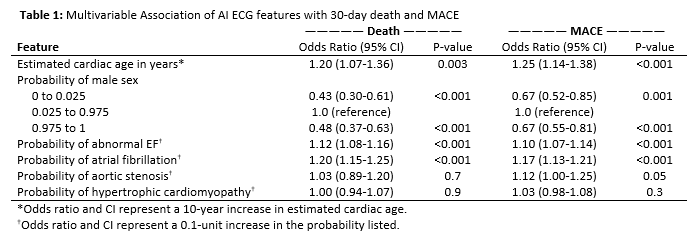
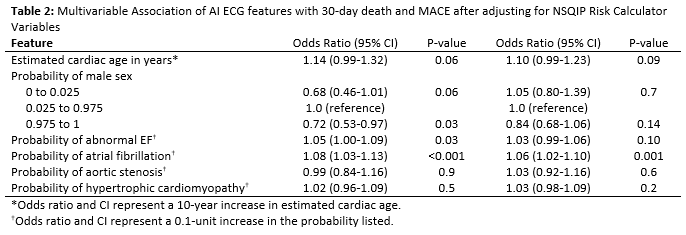
Introduction: Approximately 1% of patients undergoing non-cardiac surgery die or have a major adverse cardiac event(MACE) within 30 days. Only 20% of surgeons use online risk calculators to risk-stratify patients due to increased clinical burden. Herein, we investigate if our institution's previously created AI algorithms on pre-operative electrocardiograms(ECGs) can serve as a point-of-care risk stratification for post-operative complications. Methods: From our institutional National Surgical Quality Improvement Program(NSQIP) data, we identified 128,992 non-cardiac surgeries performed on 116,702 distinct patients between 2006-2020. We identified pre-operative ECGs within 90 days of surgery; AI algorithms were used to derive variables in(Table 1). We evaluated the relationship of AI ECG features with the following 30-day outcomes: death and MACE (stroke, cardiac event, or death). AI ECG features were evaluated in conjunction with NSQIP Surgical Risk Calculator (SRC) variables using multivariable logistic regression models to predict these outcomes, using 500-sample bootstrap-corrected c-indexes. Results: A total of 50,254(39%) surgeries(13% Urologic) had pre-operative ECGs available. The AI ECG features(Table 1) collectively had a c-index of 0.755 and 0.719, respectively, for 30-day death(n=414; 0.8%) and MACE(n=676; 1.4%). After adjusting for NSQIP SRC variables, AI ECG variables remained significantly associated with death and MACE(Table 2). The final model with AI ECG features and NSQIP SRC variables had a c-index of 0.902 death) and 0.845(MACE). Conclusions: AI features of pre-operative ECGs were significantly associated with death or MACE within 30-days of non-cardiac surgery. Clinical implementation of these algorithms to pre-operatively identify high risk surgical candidates warrants further study. SOURCE OF Funding: No sources of funding to disclose.

 photo")