Associate Professor Tokyo Medical and Dental University
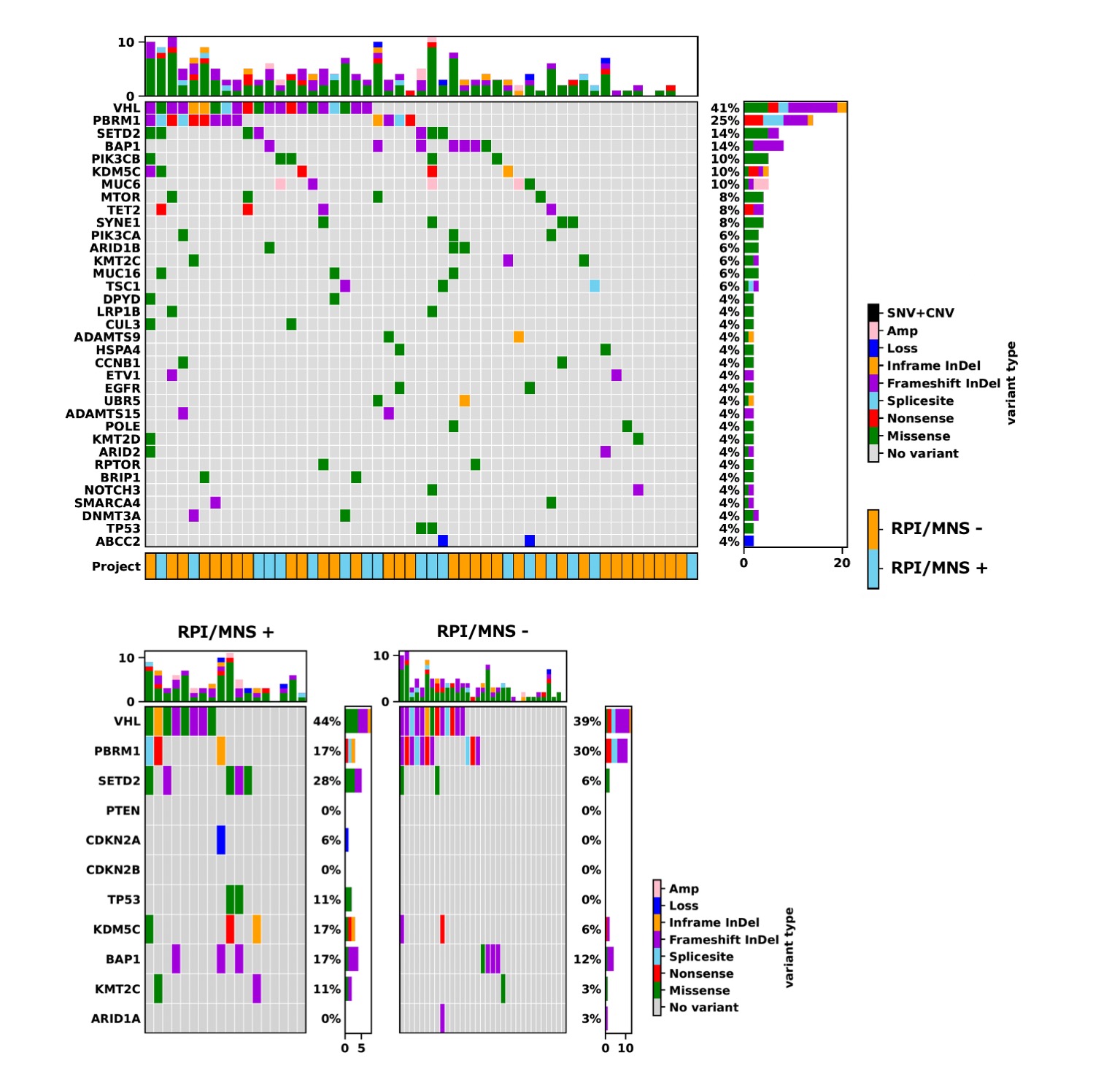
Introduction: The efficacy of adjuvant immune checkpoint inhibition has been reported recently for locally advanced clear cell renal carcinoma (ccRCC); however, further exploration is required to define optimal candidates for this strategy, who are at high risk for recurrence. In this study, we defined renal parenchymal infiltration or micronodular spread (RPI/MNS) in ccRCC and investigated its prognostic impact and genomic backgrounds. Methods: We retrospectively analyzed 333 M0 ccRCC patients treated with radical nephrectomy (approval # M2019-172 and M2021-272). Two pathologists evaluated the whole tissue sections of surgical specimens and performed the focused analysis on the tumor interface with normal renal parenchyma. Recurrence-free survival (RFS) was analyzed as an endpoint. Genomic DNA was extracted from tumor tissue in eligible cases (n=51), and variants were screened using a panel of 440 cancer-related genes. Results: Overall, =pT3a, WHO/ISUP grade 3-4, and microvascular invasion were observed in 107 (32%), 138 (41%), and 199 (60%) patients, respectively. Histological assessment revealed the variations of the tumor interface with normal renal parenchyma and identified the specific pattern at high risk for recurrence. This finding was defined as RPI/MNS, in whichcancer cells infiltrated or spread into the renal parenchyma by involving normal renal tissue and/or by forming micronodules. RPI/MNS was finally identified in 40 patients (12%). During the median follow-up of 6.0 years, 67 patients (20%) developed recurrence. On multivariable analysis, =pT3a, grade 3-4, and RPI/MNS were independently associated with shorter RFS; RPI/MNS showed the highest hazard ratio (4.63) followed by grade 3-4 (2.03) and =pT3a(1.99). 2y-RFS rates were 38% and 95% in patients with and without RPI/MNS, respectively. The genomic analysis revealed significantly different patterns of representative gene mutations in ccRCC (figure). Patients with RPI/MNS (n=18) had significantly more frequent mutations in SETD2 (28% vs. 6%) and TSC1 (17% vs. 0%) in comparison to those without RPI/MNS (n=33). Conclusions: RPI/MNS had a strong impact on recurrence after surgery with the background of aggressive genomic features in ccRCC. Adjuvant therapy may be recommended for patients showing RPI/MNS. SOURCE OF Funding: None