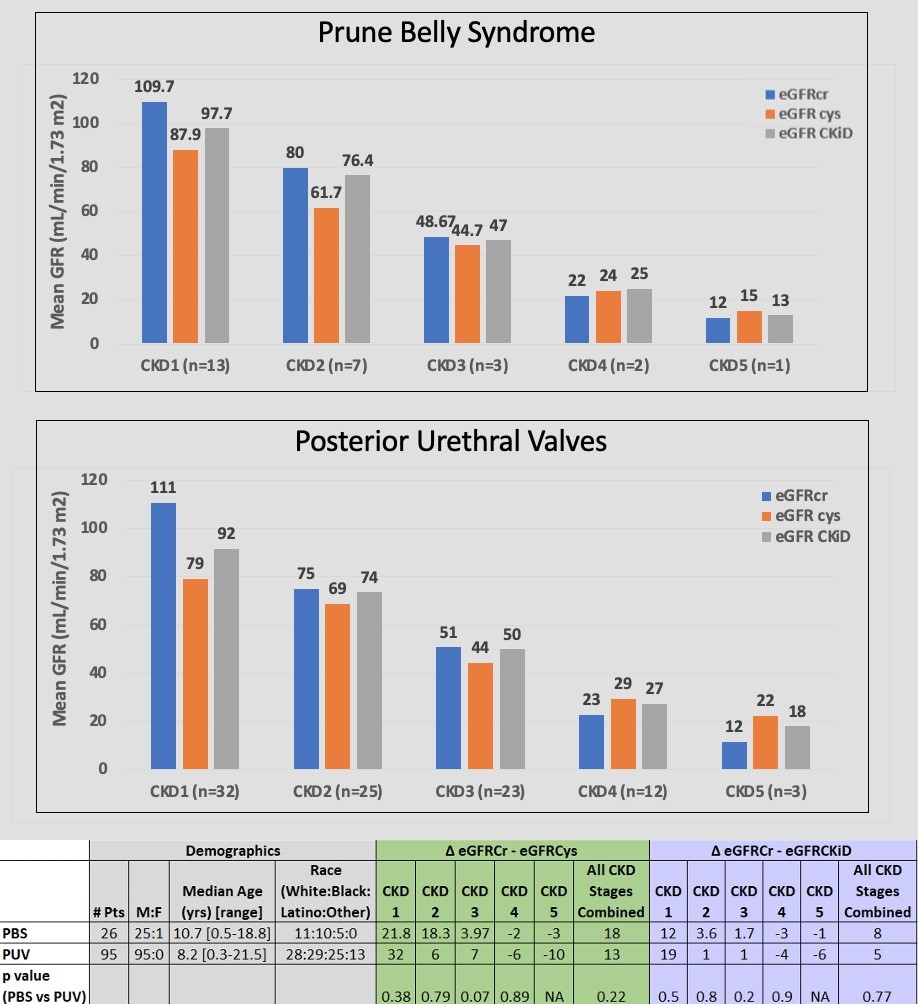
Introduction: In prune belly syndrome (PBS), prior comparison of estimated glomerular filtration rate (eGFR) with calculators using creatinine (Cr) and/or Cystatin C (Cys) showed lower mean eGFR with Cys-based calculators than with the “Bedside Schwartz” Cr-based calculator (eGFRcr) in Chronic Kidney Disease (CKD) 1 and 2. As abdominal skeletal muscle paucity in PBS could reduce serum Cr, we hypothesized the differences in mean eGFRcr and eGFR by Cys-based calculators (denoted as ?) will be greater in PBS compared to posterior urethral valves (PUV), with intact musculature. Methods: A 2014-2021 retrospective ICD-10 search identified PBS and PUV patients with labs and height without neuromuscular disorders or renal replacement. eGFRcr, eGFRcys and creatinine-cystatin C-based GFR (eGFR-CKiD) were calculated. CKD stages were assigned by eGFRcr. ? eGFRcr, eGFRcys, and eGFR-CKiD between PBS and PUV were compared with t-test. Those with normal Cr and/or Cys but who had CKD by eGFR calculators were identified. The proportion of changes in CKD staging by each calculator was compared with chi-square or Fishers exact test. Results: 95 PUV and 26 PBS patients were analyzed (Fig 1). ? eGFRCr and eGFR with Cys-based calculators by CKD stage or by all CKD stages combined were not different between PBS and PUV. By all CKD stages combined, ? eGFRcr and eGFRcys was 18 and 13 mL/min/1.73m2 in PBS and PUV, respectively (p=0.22) and ? eGFRcr and eGFR-CKiD was 8 and 5 ml/min/1.73m2 in PBS and PUV, respectively (p=0.71). Among patients with normal Cr and/or Cys, at least 25% had CKD2-3 by eGFR calculation. Changes in CKD stage by Cys-based calculators compared to eGFRcr were not significantly different between PBS and PUV (p >0.3). Upstaging was most frequent in PBS and PUV CKD1 and 2. Conclusions: Differences between eGFRcr and eGFR by Cys-based calculators in PBS and PUV patients were not significant, suggesting paucity of abdominal musculature in PBS may not account for the lower eGFRs observed using Cys-based calculators. In 25% of patients, normal Cr and/or Cys actually had CKD2-3, highlighting importance of eGFR calculation. Cys-based calculators upstaged, especially in CKD1 and 2. Cys-based eGFRs calculators should be considered for early identification of CKD in patients with congenital urologic abnormalities prone to renal dysfunction. SOURCE OF Funding: None