Session: PD24: Kidney Cancer: Advanced (including Drug Therapy) II
PD24-05: Complete Pathological Response in Patients Undergoing Nephrectomy for Renal Cell Carcinoma Following Immune Checkpoint Inhibitor Therapy: A Multicenter Study
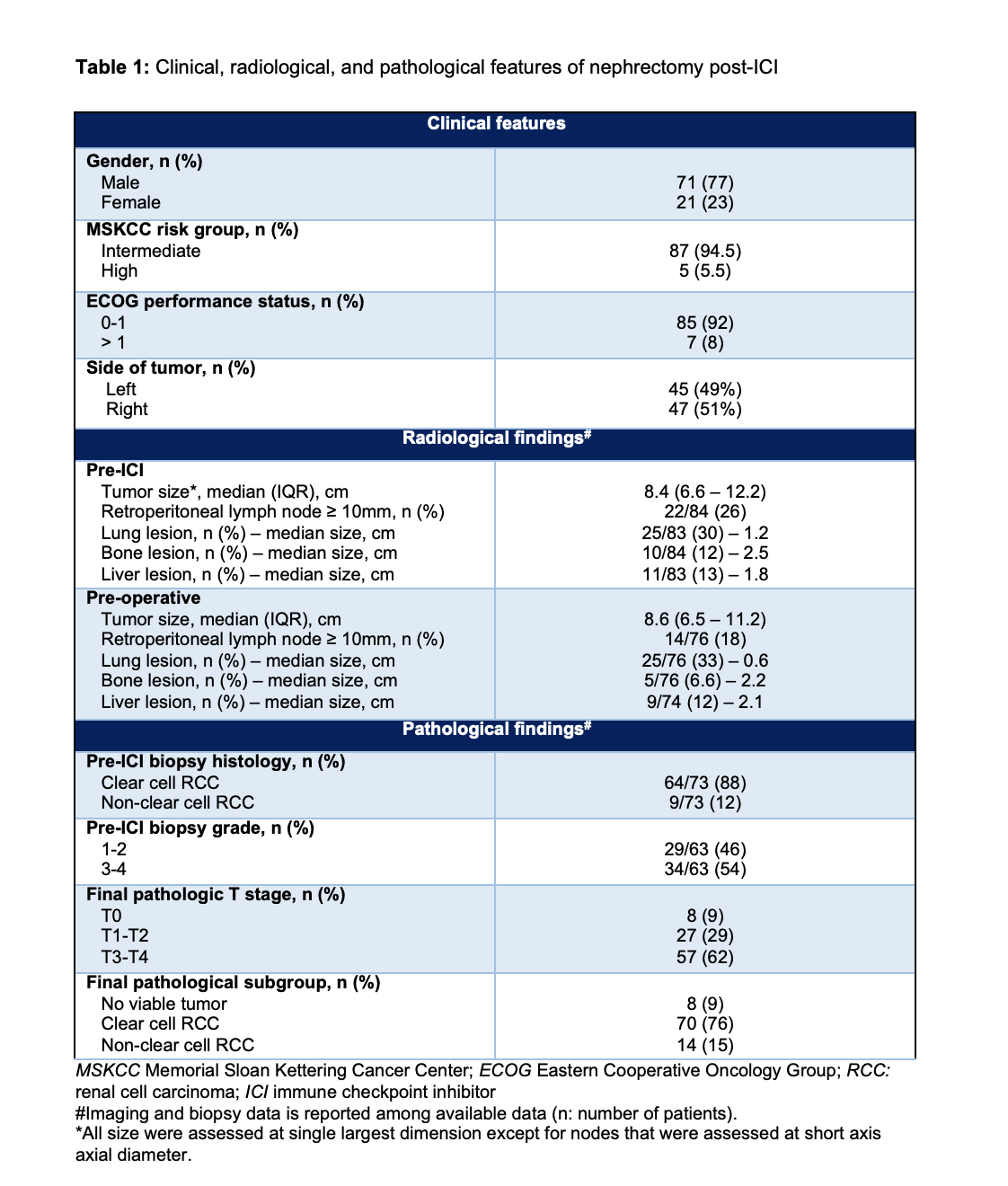
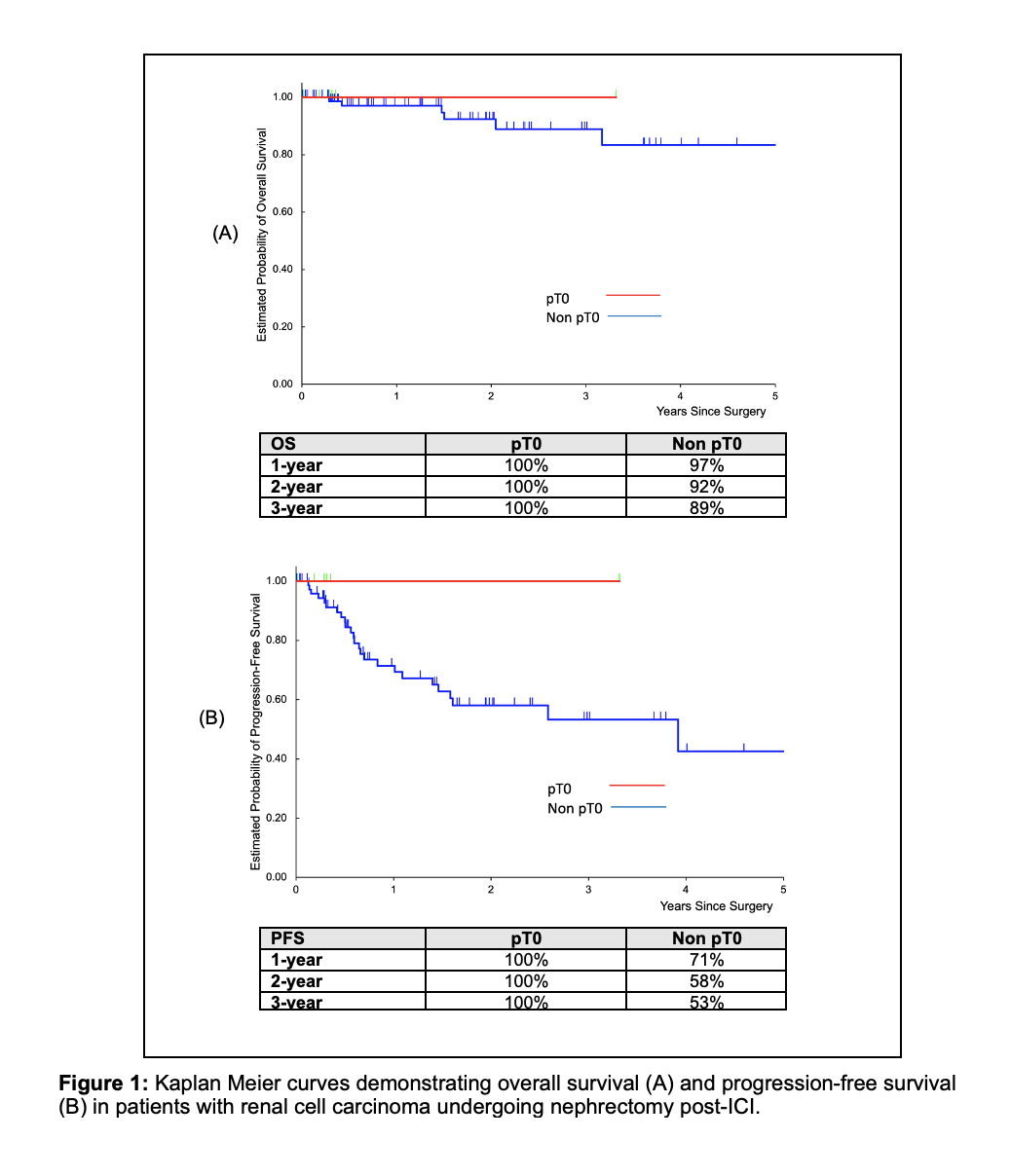
Introduction: Immune checkpoint inhibitors (ICI) are now among frontline treatments for advanced renal cell carcinoma (RCC). The aim of this study is to evaluate predictors and outcomes of patients with complete pathologic response in the primary tumor following ICI therapy. Methods: Patients with RCC undergoing nephrectomy following ICI therapy were evaluated in three high-volume US academic centers. Available pre-ICI and preoperative computed tomography imaging were reviewed by expert radiologists. Radiological data, clinical features, and outcomes of patients with and without complete pathological response were compared. Results: A total of 92 patients with a median (IQR) age of 63 (56-69) years were included. Among patients with available data, ICI regimens (median cycles=3) were Nivolumab ± Ipilimumab (n=76), and Pembrolizumab ± Axitinib (n=12). Clinical, radiological, and pathological features of the patients are shown in table 1. Among all patients, 90 (98%) underwent radical and 2 (2%) partial nephrectomy; 40 (43.5%) open, 40 (43.5%) robotic and 12 (13%) laparoscopic. Median operative time, estimated blood loss, and length of stay were 3 hours, 200 mL, and 3 days, respectively. Eight patients (9%) showed complete pathological response in the kidney. Complete pathological response was marginally associated with higher number of ICI cycles (> 3 vs. = 3 cycles: 16% vs. 4%, p = 0.06), and with no other clinical or pretreatment radiologic variable. 3-year overall and progression-free survivals in patients with complete pathological response were 100%; however, the same outcomes in other patients were 89% and 53%, respectively (Figure 1). Conclusions: In our cohort, 9% of patients who underwent nephrectomy following immune checkpoint inhibitors for advanced RCC showed complete pathological response in nephrectomy specimen. These patients demonstrated more favorable overall and progression-free survivals compared to those with residual tumor in the final specimen. SOURCE OF Funding: None

 photo")