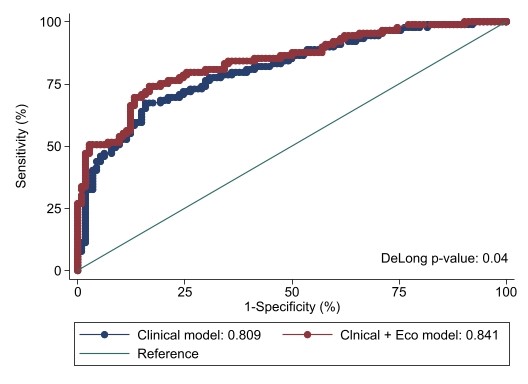
Introduction: Stratification of patients with localized prostate cancer (PCa) before robotic assisted radical prostatectomy (RARP) allows performing a tailor-made surgery, potentially providing a nerve-sparing procedure even in those patients with high-risk disease. Nowadays the accuracy of clinical parameters to determine extraprostatic extension (EPE) is moderate, so a new imaging tool capable of providing a more accurate assessment is in order. Our goal is to evaluate the added value of microUS in the preoperative prediction of EPE. Methods: Our prospective single-institutional cohort study enrolled patients with diagnosis of PCa scheduled for RARP. We included patients with PSA <20 ng/mL, prostate volume <100 mL and a preoperative microUS investigation. MRI-derived features (curvilinear contact length [CCL], capsular bulging, visible extracapsular extension [ECE]), along with microUS features (such as the presence of hypoechoic halo and obliteration of the vesicle-prostatic angle) were tested as predictors of EPE. Multivariable logistic regression models were fitted to test the accuracy of clinical parameters (total PSA, ISUP biopsy and digital rectal examination [DRE]) plus microUS parameters for EPE prediction. Results: Overall, 230 patients were recruited. All predictors were associated with non-organconfined disease (p < 0.001). Histological findings showed that 131 (56.9%) and 99 (43.0%) had respectively a pT2 and a pT3 or greater disease. Individuals with only 1 predictor had a rate of non-organconfined PCa of 16.7% (OR 3.12), compared to 93.8% in those where 4 predictors were simultaneously observed (OR 75.0). At MLRM, the most significant risk factors for EPE were visible ECE (OR 3.23; p<0.004), positive DRE (OR 2.5;p=0.015), and PSA (OR 1.06; p=0.03). The AUC increased from 0.809 to 0.841 when considering the clinical model alone and the model including both clinical and microUS features respectively (Figure1). The DeLong test for equality showed a significant difference between the two curves (p=0.04). Conclusions: Our results confirm that microUS may represent an accurate tool for the evaluation of non-organ confined PCa. Future studies should externally validate our findings and determine the impact of microUS in the outcomes of RARP. SOURCE OF Funding: None

 photo")