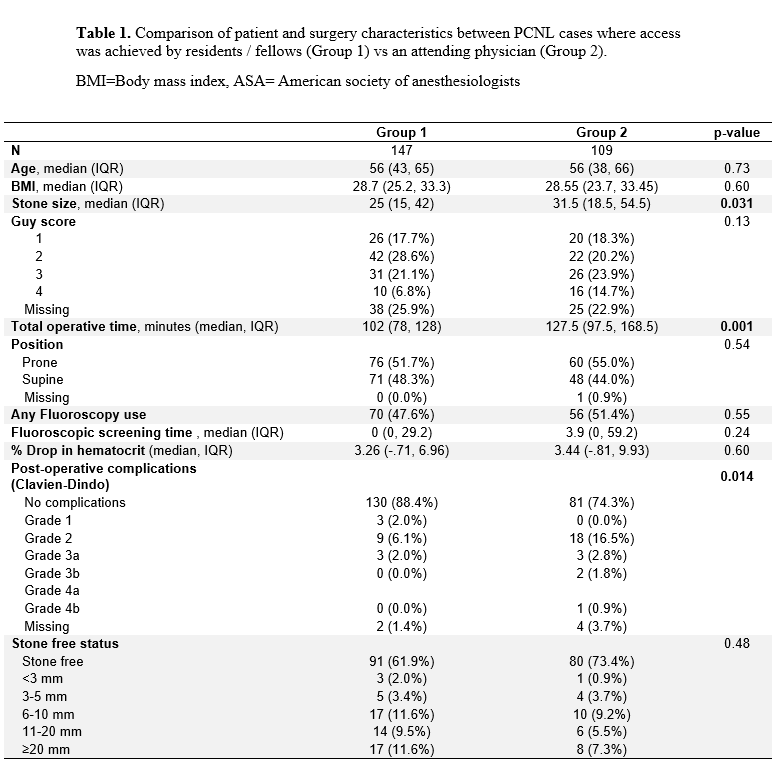
Introduction: Use of percutaneous nephrolithotomy (PCNL) is now standard for stones larger than 20 mm by the American Urological Association guidelines. Achieving percutaneous access is a critical step of successful PCNL, and it is important for urologists to learn this skill to provide patients with the highest quality stone care. We aimed to assess clinical outcomes in PCNL cases in which access was achieved by trainees versus attending physicians to examine whether access obtained by surgeons early in their learning curve was safe. Methods: Prospectively collected data from the Registry for Stones of the Kidney and Ureter (ReSKU) was reviewed for all patients who underwent PCNL at a single center between 2015 and 2021. The level of expertise of the surgeon acquiring access was recorded in all cases and categorized as obtained by the resident, fellow, or attending physician. Stone characteristics were analyzed; stone burden was calculated using maximal summative diameter. Primary outcomes were Clavien-Dindo post-operative complications and stone free status. Univariate statistics were used to compare outcomes between Group 1 (cases where access was achieved by a trainee (resident or fellow)) and Group 2 (cases where access was achieved by an attending). Results: 256 PCNL cases with follow-up data were included in the analysis. Percutaneous access was obtained by a trainee in 147 (57.4%) cases and by an attending physician in 109 (42.6%) cases. Median stone burden was 29 mm (IQR 16 – 48 mm) and 32.4% of stones were Guy complexity score 3 or 4. Comparison of stone and patient characteristics is demonstrated in Table 1. Cases in Group 1 had a smaller median stone size and shorter operative time. Patient positioning and use of fluoroscopy (52.4% ultrasound only in group 1 vs 48.6% in Group 2) were similar between groups. Stone free status was not statistically different between groups (61.9% in group 1 vs 73.4% in group 2, p=0.48), but there were more Clavien-Dindo 2A complications in Group 2 (6.1% in group 1 vs 16.5% in group 2) (p=0.014). Conclusions: Percutaneous access achieved by trainees earlier in their learning curve compared to experienced attending surgeons appears to be safe. These data support the idea that with careful patient selection, urologists can safely acquire this important surgical skill. SOURCE OF Funding: None