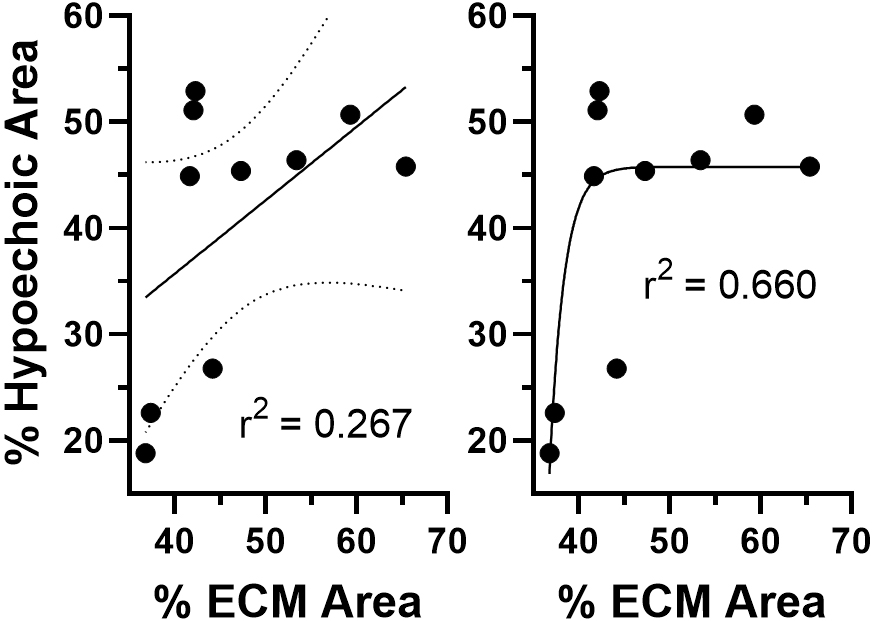
Introduction: Previous studies have shown that pre-operative in-office erectile function testing (pharmacocavernosometry) was correlated with erectile tissue composition (ETC) as determined by color histomorphometry on tissue samples removed during penile prosthesis insertion. Corporal veno-occlusive function (CVOF) was found to be normal at 45-50% smooth muscle cell content (SMCC). CVOF significantly worsened in an exponential relationship when SMCC was 40-25%. Below 25% SMCC, there was no recordable CVOF. We previously reported that using Grayscale pharmaco-ultrasonography (GPUS), a less invasive diagnostic assessment for ED than pharmacocavernosometry, % hypoechoic area (HA) in the corpora cavernosa (CC) negatively correlates with the erectile function domain score of the IIEF. In this study, we examined the relationship between % HA on GPUS and ETC in men with ED. Methods: Pre-operative proximal shaft axial plane GPUS images were obtained using a 15.4 MHz probe (Aixplorer), gain setting 45%, dynamic range 70dB. % HA within the CC was assessed by computer-assisted image analysis using Image J. During penile prosthesis surgery, CC tissue from the proximal shaft was biopsied for histological analysis (n=10). Formalin-fixed (10%), paraffin-embedded tissue sections (5 µm) were stained with Masson’s trichrome. Photomicrographs were also analyzed by Image J using the Masson trichrome vector of the color deconvolution plugin. ETC was determined by assessing fractional areas of cellular content, consistent with SMCC, and extracellular matrix (ECM), consistent with erectile tissue fibrosis, from the red and blue channels, respectively. Results: % HA was poorly correlated to % ECM area by linear regression analysis (r2 = 0.267). However, a non-linear regression model (exponential growth curve) provided a better fit (r2 = 0.660) with an inflection point at 40% ECM (see Figure). The abrupt shift is similar to the previously reported CVOF curve using pharmacocavernosometry. Conclusions: Estimation of % HA on GPUS images may be a useful, non-invasive assessment of ETC. Larger cohorts of ED patients are needed to verify the clinical utility of GPUS to predict CVOF. SOURCE OF Funding: None