Session: MP28: Kidney Cancer: Advanced (including Drug Therapy) I
MP28-08: Outcome change in patients with advanced renal cell carcinoma outside of clinical trials from the tyrosine-kinase inhibitor era to the immune checkpoint inhibitor era
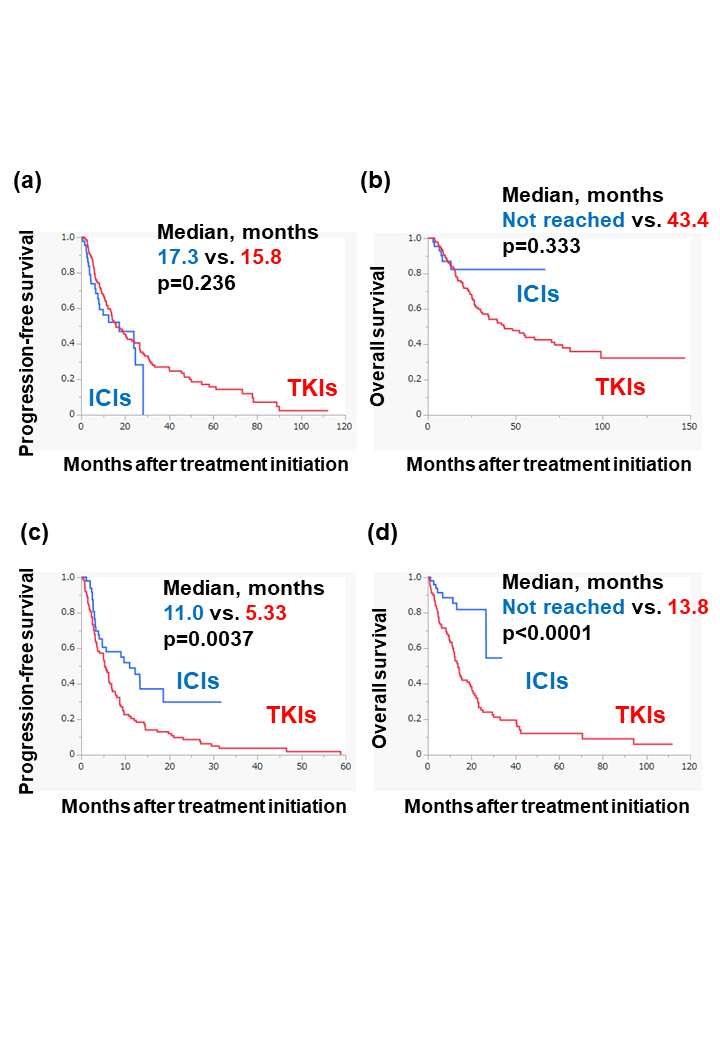
Introduction: Clinical trials have demonstrated the superior efficacy of immune checkpoint inhibitor (ICI)-based combination therapy over sunitinib, a multi-target tyrosine kinase inhibitor (TKI), in patients with advanced renal cell carcinoma (RCC). However, such benefit has not been elucidated in populations outside of clinical trials. Methods: We retrospectively evaluated data of 331 patients with advanced RCC receiving ICI-based combination therapy or TKIs as first-line therapy. Patients were determined as trial-ineligible when at least one of following factors was present: KPS score <70%, hemoglobin level <9.0 g/dL, eGFR <40 mL/min/1.73 m2, platelet count <100,000/µL, neutrophil count <1500/µL, non-clear cell histology, or brain metastasis. The outcome change from the previous TKIs to the current ICI-based combination therapy was analyzed in both trial-eligible and trial-ineligible populations. Results: This study included 48/93 (52%) and 101/238 (42%) patients receiving TKI and ICI-based combination therapy outside of clinical trials, respectively. Among the TKI-treated patients, the trial-ineligible patients had significantly lower progression-free survival (PFS) (p < 0.0001) and overall survival (OS) (p < 0.0001) than the trial-eligible patients. In contrast, among ICI-based combination therapy-treated patients, no significant difference in PFS (p=0.393) or OS (p=0.634) was found between them. On analyzing each population based on trial eligibility throughout the TKI and ICI-based combination therapy, in the trial-eligible population, no significant difference in PFS (p=0.236) or OS (p=0.333) was found between TKI and ICI-based combination therapy (Figure a and b). However, in the trial-ineligible population, PFS (p=0.0037) and OS (p < 0.0001) were significantly higher for the ICI-based combination therapy than for the TKIs (Figure c and d). Conclusions: Using real-world data, this study indicated the substantial rate of patients with advanced RCC treated with systemic therapy outside of clinical trials. ICI-based combination therapy helped improve outcomes of advanced RCC, and the therapeutic benefit was more prominent in the trial-ineligible population than in the trial-eligible population. SOURCE OF Funding: None.