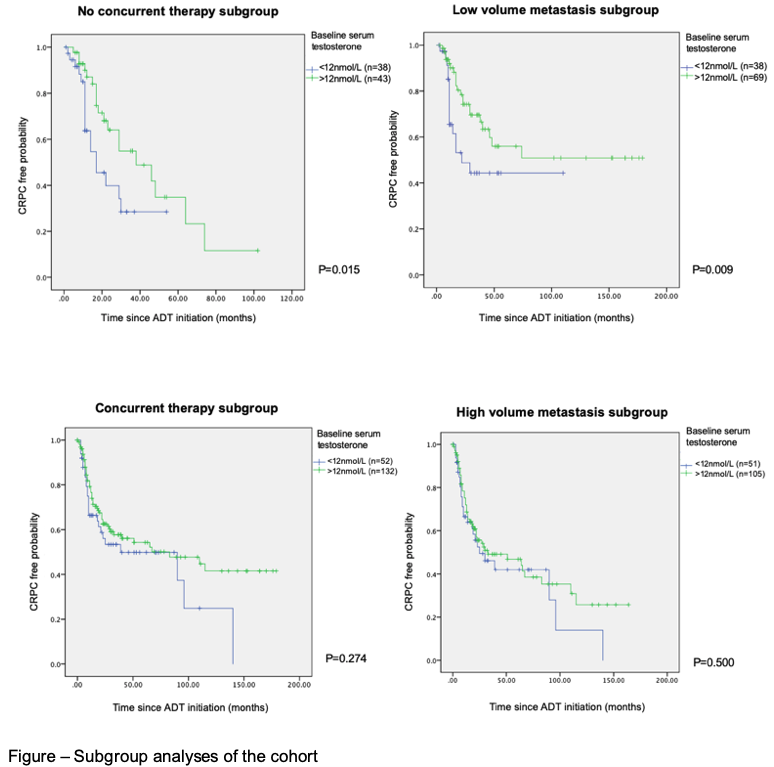
Introduction: Androgen deprivation therapy (ADT) is key to the treatment of metastatic prostate cancer (mHSPC). The evidence of baseline testosterone prior to ADT on mHSPC outcomes is scarce in the era of concurrent therapy. We aim to investigate the effect of baseline testosterone on time to castration resistant prostate cancer (CRPC) in a cohort of mHSPC. Methods: This is a multicentre review of prospectively maintained databases from China, Japan, Austria and Spain, including patients with pre-ADT testosterone levels. 249 cases of mHSPC with ADT initiated from 2002 to 2021, with histologically proven Ca Prostate were analysed. Baseline testosterone was divided into high and low with a cutoff of 12 nmol/L. Kaplan-Meier was used to evaluate the correlation between baseline testosterone level and time to CRPC. Subgroup analysis was performed to elucidate the effect of volume of metastasis (by criteria adopted in CHAARTED trial) and use of concurrent treatment (use of chemotherapy or novel hormonal agent at the beginning of ADT). The primary outcome is time to CRPC (PSA progression of >25% rise above the nadir). Results: The median age was 71 (IQR 10). Median follow up time was 30 months. Median pre-ADT PSA level was 156 ng/mL. The portion of cases of ISUP grade 1-3, 4 and 5 respectively was 6.3%, 30.8% and 62.9%. 150 patients (60.2%) had high volume metastasis at diagnosis. 170 patients (67.7%) received concurrent therapy. 115 patients (45.8%) developed CRPC at the end of data collection. The mean time to CRPC of the cohort is 20.0 months (SEM: 2.1). Overall there was no correlation between baseline testosterone and time to CRPC. In the subgroup of cases without concurrent therapy, a lower baseline testosterone level was associated with significantly shorter time to CRPC (p=0.015), so was in the subgroup of low volume metastasis (p=0.009). In the subgroup of high volume metastasis or men with concurrent therapy, baseline testosterone was not associated with time to CRPC. Conclusions: In low volume mHSPC or in the absence of concurrent therapy, a lower baseline testosterone level was associated with shorter time to CRPC. Pre-treatment testosterone level may predict prognosis in mHSPC. mHSPC patients with low baseline testosterone should be encouraged to use concurrent therapy to delay progression to CRPC. SOURCE OF Funding: Nil