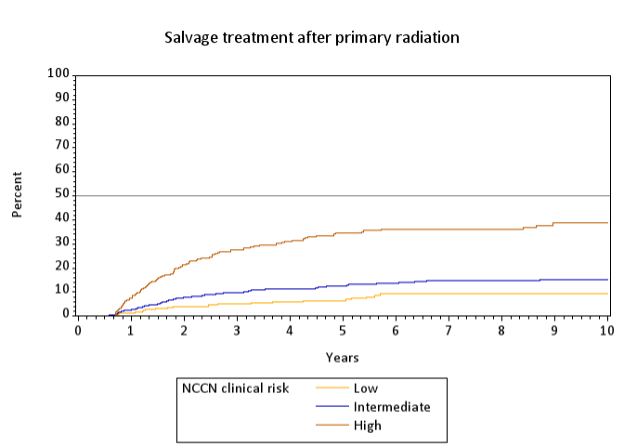
Introduction: Radiation therapy is a common form of treatment for men with prostate cancer. Biochemical recurrence (BCR) is defined according to the ASTRO Phoenix definition of PSA nadir + 2. We sought to characterize long term rates of biochemical recurrence in a large, well-characterized and well-followed cohort of men treated with primary external beam radiation therapy (EBRT). Methods: Patients were enrolled in CaPSURE, a national registry of men diagnosed with prostate cancer, from 1995 - 2017 with clinically localized prostate cancer (cN0M0/X, PSA<=50) and treated with primary EBRT. Cancer risk was defined by NCCN criteria. Cox proportional hazards regressions were used to assess associations between patient characteristics and BCR was defined by PSA nadir + 2. Results: 1193 patients were included. Mean age at diagnosis was 70 (SD 6.82), median PSA at diagnosis was 7.5 and mean number of follow up PSA tests was 5. Overall rates of BCR were 17.4% at 5 years and 39.4% at 10 years. NCCN clinical risk was significantly associated with rates of BCR with high-risk patients having the highest rates of recurrence, followed by intermediate- and low-risk groups (61.5%, 36.4% and 28.5% respectively at 10 years, log-rank p<0.01). NCCN high vs low clinical risk was significantly associated with likelihood of BCR (HR 4.8, CI 2.5 – 9.2). Rates of salvage treatment were 16% at 5 years and 19% at 10 years and these were also significantly associated with NCCN high vs low clinical risk (HR 3.7, CI 2.3 – 6) and concurrent ADT (HR 1.83, CI 1.2 – 2.7). Overall rates of bone metastases were 2.6% at 5 years and 4% at 10 years. Overall prostate cancer specific mortality was 3% at 5 years and 7% at 10 years. Conclusions: In this analysis, rates of BCR were fairly high and consistent with published RTOG studies, but rates of salvage treatment were relatively low in comparison, indicating that not all patients who recur need, are offered or want treatment. The limitations of this analysis include incomplete information on radiation dose and field size. The strengths of this analysis include the size of the cohort and the length of follow-up. Furthermore, as this cohort largely represents treatment in community settings, the results may be broadly applicable. SOURCE OF Funding: UCSF Goldberg-Benioff Program in Translational Cancer Biology