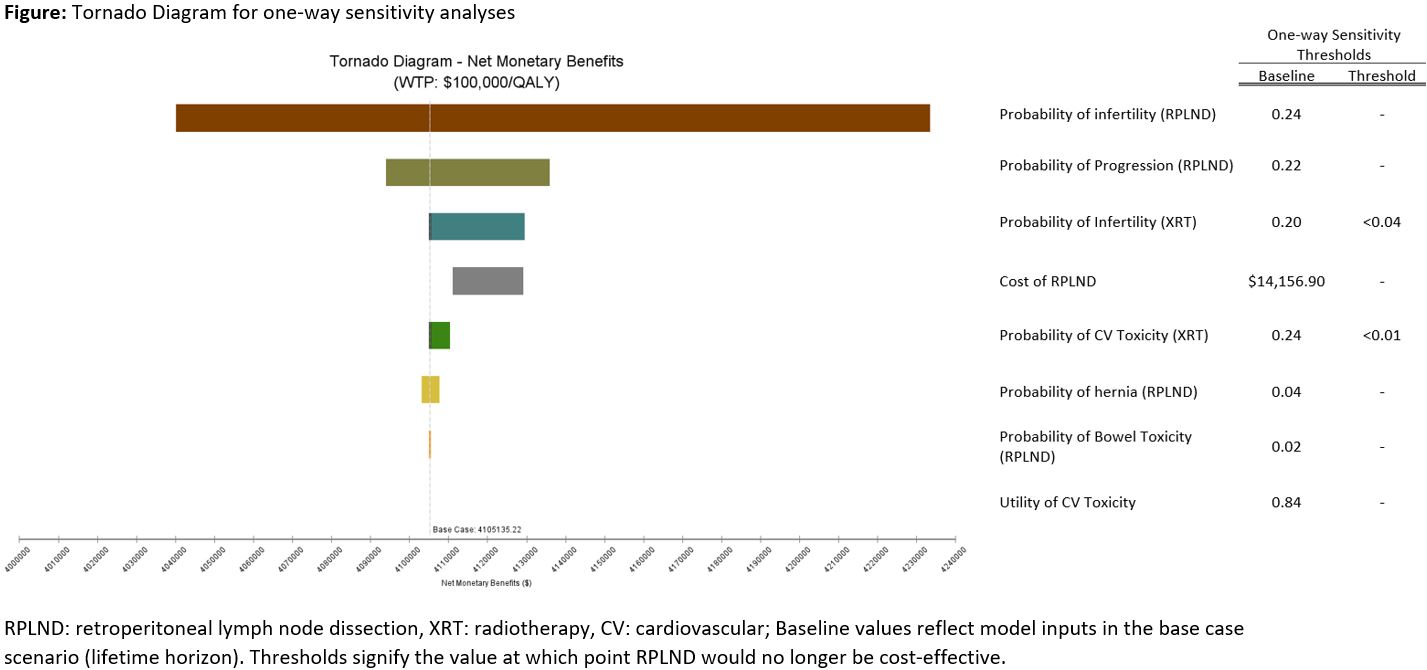
Introduction: The recent Surgery in Early Metastatic Seminoma (SEMS) trial examined retroperitoneal lymph node dissection (RPLND) as a first-line treatment for patients with isolated 1-3cm retroperitoneal lymphadenopathy. To date, the standard of care for these patients has been either chemotherapy or radiation (XRT). Herein, we evaluated the relative cost-effectiveness of these management strategies. Methods: A decision-analytic Markov model was used to assess cost-effectiveness of RPLND, chemotherapy (3 cycles of cisplatin, etoposide, bleomycin), and XRT for management of stage IIA seminoma. Probabilities of progression for RPLND were obtained from SEMS trial presented abstract data. All other probability and utility values were obtained from published literature. Analyses were performed with a 3-month cycle for a lifetime horizon. Primary outcomes included costs from a commercial insurer’s perspective, effectiveness (quality adjusted life years, QALY), and incremental cost-effectiveness ratios (ICER). A willingness to pay threshold of $100,000/QALY was used. Sensitivity analyses were performed to evaluate model robustness. Results: At a lifetime horizon, the mean costs per patient for RPLND, XRT, and chemotherapy were $41,291, $75,650, and $85,380, respectively. The mean QALYs per person were 41.65, 41.62, and 39.60 for RPLND, XRT, and chemotherapy, respectively. RPLND was found to be the most cost-effective approach due to high costs and the accrued disutility of chronic toxicities associated with both XRT (ICER: -$107,296/QALY) and chemotherapy (ICER: -$26,941/QALY). On one-way sensitivity analyses (Figure), RPLND was no longer cost-effective if the probabilities of infertility and cardiovascular toxicity after XRT were less than 4% and 1%, respectively. Conclusions: RPLND was the least costly and most effective treatment strategy for stage IIA seminoma. In particular, long-term toxicity costs and disutilities associated with chemotherapy and XRT resulted in lower cost-effectiveness for these two approaches. These findings support clinical guideline consideration of including RPLND as a treatment option for well selected patients with stage IIA seminoma. SOURCE OF Funding: None