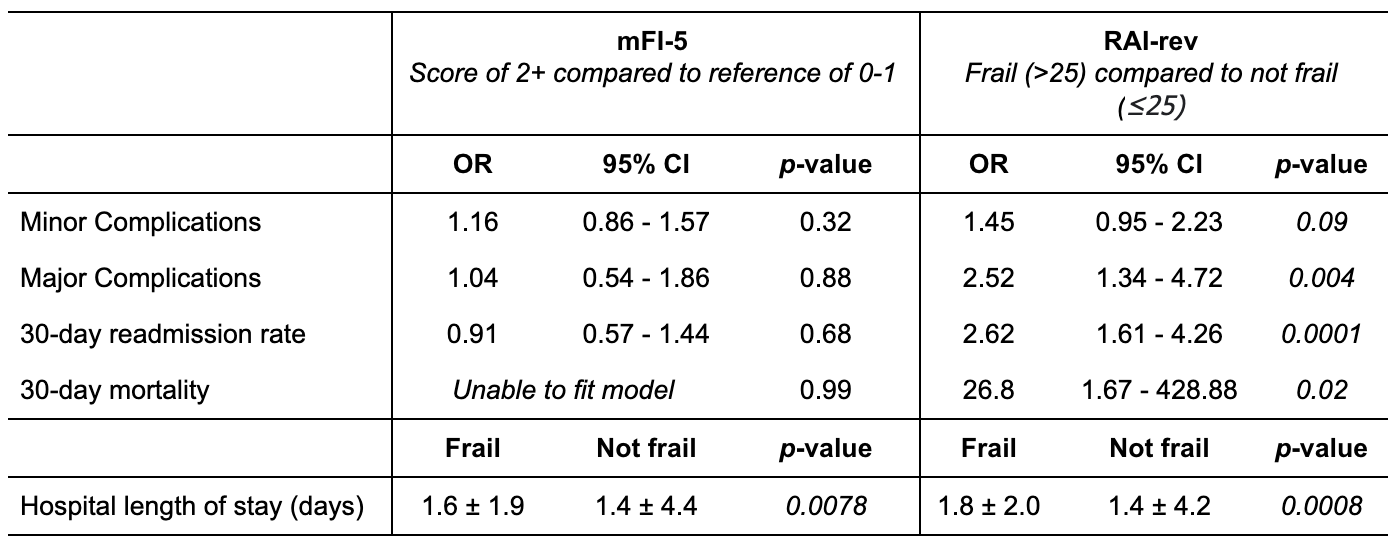
Introduction: Sacrocolpopexy (SCP) is a definitive treatment option for pelvic organ prolapse (POP). Because there are less invasive, albeit less definitive treatment options, a frailty index that best predicts outcomes and mortality for patients desiring SCP is useful to aid in decision making. Methods: Open and minimally invasive SCPs performed from 2006 to 2020 were identified inthe National Surgical Quality Improvement Program (NSQIP) database. Frailty was determined by the NSQIP modified frailty index (mFI-5), a validated 5-item score including points for diabetes, impaired functional status, COPD, CHF, and hypertension, and by the revised surgical Risk Analysis Index (RAI-rev), a validated score accounting for patient comorbidities, age, and functional status. As previously published, patients with mFI-5 scores of 2 or more and RAI-rev scores of 26 or more were considered “frail.” Univariate logistic regression and t-test analyses were performed for mFI-5 and RAI-rev as predictors of surgical complications, 30-day readmissions, 30-day mortality, and hospital length of stay (LOS). Results: 9,082 SCPs were identified in the database. In total, 5.2% of patients experienced minor complications (superficial SSIs, pneumonia, UTIs, bleeding requiring transfusion, or AKIs), and 1.4% of patients experienced major complications (sepsis, DVT, stroke, reintubation, renal failure, myocardial infarction, pulmonary embolism, septic shock, wound dehiscence, deep wound infections, or cardiac arrest). The 30-day readmission and mortality rates were 2.7% and 0.02%, respectively. On univariate logistic regression, a frail mFI-5 score was not predictive of minor complications, major complications, 30-day readmissions or mortality. However, a frail compared to a non-frail mFI-5 was associated with a higher LOS (1.6 vs 1.4, p=.008). A frail compared to a non-frail RAI-rev was predictive of major complications [OR 2.52; 95%CI 1.34-4.72; p=0.004], 30-day readmissions [OR 2.62, 95%CI 1.61-4.26; p=.0001], 30-day mortality [OR 26.8; 95%CI 1.67-428.88; p=0.02], and LOS (1.8 vs 1.4 days, p=.0008). Conclusions: The RAI-rev is a better predictor than the mFI-5 for major complications, readmission rate, mortality, and hospital LOS and may help in the decision making and risk counseling for patients POP considering an SCP. SOURCE OF Funding: n/a