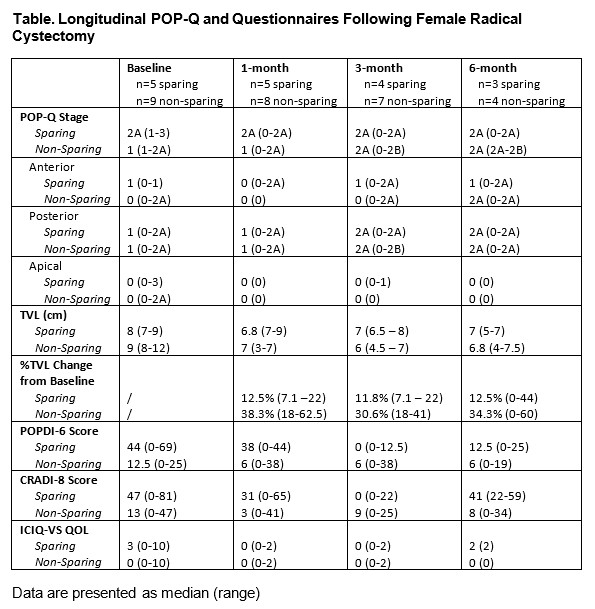
Introduction: Women are at risk of pelvic organ prolapse and sexual dysfunction following radical cystectomy (RC); however, these outcomes are under-appreciated and understudied. We aimed to assess the natural history of pelvic floor support and vaginal symptoms following female RC. Methods: This is an interim analysis of an IRB-approved multicenter prospective observational study of pelvic floor support in women undergoing RC from 3/2021 to 5/2022. All women undergoing RC at 2 institutions were recruited. Participants underwent pelvic exam including Pelvic Organ Prolapse Quantification System (POP-Q) measurements by an FPMRS-trained urologist at baseline and routine postoperative visits. Participants completed validated questionnaires (Pelvic Floor Disability Index (PFDI-20); International Consultation on Incontinence Questionnaire Vaginal Symptoms (ICIQ-VS)) at each visit. Surgical details including amount of vaginal tissue removed during non-vaginal-sparing RC were recorded. Results: Fourteen women enrolled and had at least one postoperative visit through 6-months. Median age was 69 years. Approach was robotic in n=9 (64%) and vaginal-sparing in n=5 (38%). Indication was benign for 3 patients and all underwent non-orthotopic diversion. One vaginal-sparing benign case had concomitant mesh sacrocolpopexy for baseline stage 3 apical prolapse, while one patient from sparing and non-sparing groups had concurrent uterosacral ligament plication. All non-vaginal-sparing cases had clamshell reconstruction following excision of a median of 4.0 [4.0, 6.0] cm length and 2.5 [2.0, 4.0] cm width vaginal tissue, representing median 48% of baseline total vaginal length removed. Table 1 illustrates longitudinal POP-Q exam and questionnaire scores of vaginal sparing and non-sparing cases. One patient had anterior vaginal wall dehiscence requiring debridement under anesthesia but ultimately not reconstruction. Conclusions: To our knowledge, this is the first prospective study of pelvic floor support following female RC. Though further study is needed, preliminary findings through 6-month follow-up suggest vaginal foreshortening in both vaginal-sparing and non-sparing cases. Both groups appear to have mild anterior/posterior prolapse progression, although without worsened symptom scores. SOURCE OF Funding: None