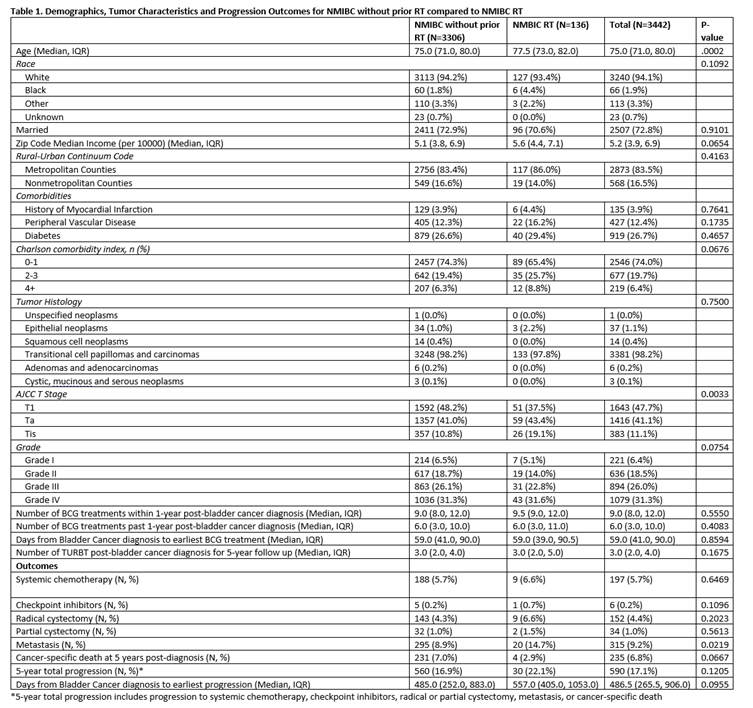
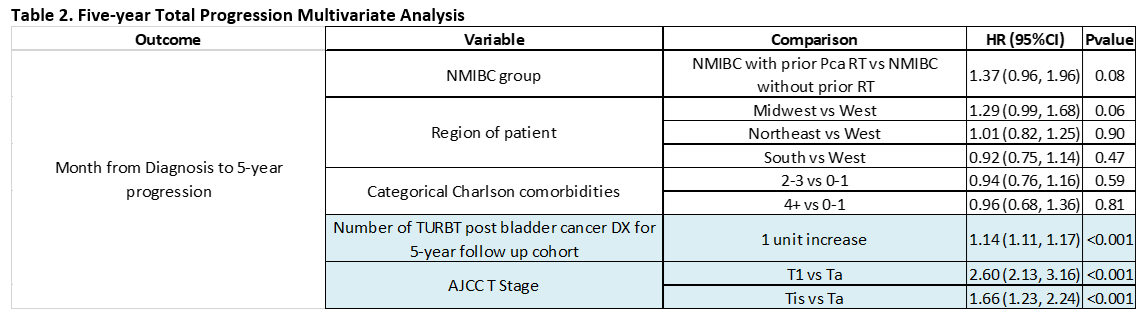
Introduction: There is evidence that patients with bladder cancer who have previously received radiation therapy (RT) are at increased risk for poorer oncological compared to non-radiated counterparts. Little is known about the impact of prior RT on the efficacy of Bacillus Calmette-Guerin (BCG) in patients with non-muscle invasive bladder cancer (NMIBC). In this context, we investigated the impact of previous prostate RT on 5-year disease progression for NMIBC patients after BCG. Methods: Male patients with a history of high-risk NMIBC, classified as Ta, T1 and CIS disease with completion of adequate BCG (at least 5 plus 2 treatments), were identified in the Surveillance, Epidemiology, and End Results (SEER) – Medicare database. Patients were stratified into two cohorts based on their history of prior radiation use: RT for prostate cancer prior to bladder cancer diagnosis (NMIBC RT) and no history of prostate cancer radiation (NMIBC without prior RT). The primary endpoint was 5-year total progression defined as progression to systemic chemotherapy, checkpoint inhibitors, radical or partial cystectomy, metastasis or cancer-specific death. Results: In a total of 3442 patients with NMIBC, 3306 had no history of prior RT while 136 had a history of prior RT for prostate cancer. The NMIBC RT cohort varied significantly by age (77.5 v 75.0, p = 0.0002) and stage (Ta 43.4%, Tis 19.1%, T1 37.5% v Ta 41.0%, Tis 10.8%, T1 48.2%, p = 0.0033) at initial tumor diagnosis. There was no significant difference in risk of progression to chemotherapy (p = 0.6469), checkpoint inhibitors (p = 0.1096), radical cystectomy (p = 0.2023), partial cystectomy (p = 0.5613), cancer-specific death (p = 0.0667) and 5-year total progression between the two cohorts. On multivariate analysis NMIBC RT patients did not have a significantly higher risk of 5-year total progression (HR 1.37, p = 0.08). Conclusions: In patients with NMIBC who undergo adequate BCG treatment, prior history of pelvic radiation for prostate cancer is not associated with worse progression-free survival. SOURCE OF Funding: This study was supported by Grant Number P30 CA015083 from the National Cancer Institute (NCI) and from the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery (M.D.T.), the Christian Haub Family Career Development Award for Cancer Research Honoring Dr. Richard Emslander (M.D.T.), and the Eric and Gail Blodgett Foundation (M.D.T.). Its contents are solely the authors' responsibility and do not necessarily represent the official view of the NIH.