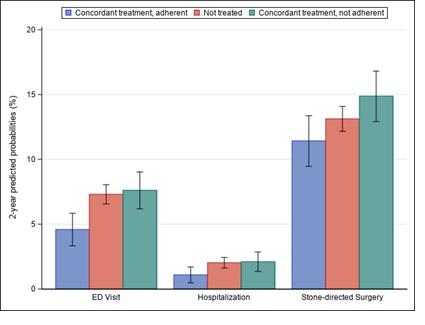
Introduction: Most efficacy results supporting preventive pharmacological therapy (PPT) used to reduce kidney stone recurrence are based on composite outcomes largely driven by imaging findings. Because these findings are surrogates for things about which patients and their clinicians care, we conducted an observational study to determine whether PPT use led to fewer symptomatic kidney stone events, requiring emergency department (ED) visit, hospitalization, or surgery. Methods: We identified a cohort of Medicare enrollees who had a 24-hour urine collection processed by a large central laboratory (2011-2016). We linked their clinical data with their pharmacy and medical claims. Among the subset with at least one biochemistry abnormality, we distinguished those who were prescribed guideline-concordant PPT (i.e., thiazides for hypercalciuria, alkali citrate therapy for hypocitraturia or low urine pH, uric acid lowering agents for hyperuricosuria) from those who were not. We differentiated between adherent and nonadherent PPT users based on the proportion of days covered method. We fit multivariate Cox models to estimate the hazard of a symptomatic stone event as a function of PPT use. Results: In total, 7,230 patients met criteria, 55% of whom had hypocitraturia. Sixty-nine percent were untreated, and 31% were prescribed concordant PPT (alkali citrate therapy was used in 66%). Compared to untreated patients, those prescribed concordant therapy and adhered to their medication had a 38% lower hazard of ED visit (P <0.01) and a 46% lower hazard of hospitalization (P=0.04). Put differently, compared to untreated patients, concordant/adherent patients had lower 2-year predicted probabilities of ED visit (4.6% vs. 7.3%) and hospitalization (1.1% vs. 2.0%) (P <0.05 for each comparison). A similar pattern was noted for stone directed surgery but was not significant (Figure). Conclusions: Our findings help strengthen the evidence base for PPT use, providing real-world data on its clinical effectiveness. SOURCE OF Funding: Dr. Hollingsworth's research is funded by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases R01DK121709.