New York Presbyterian - Weill Cornell Medical Center
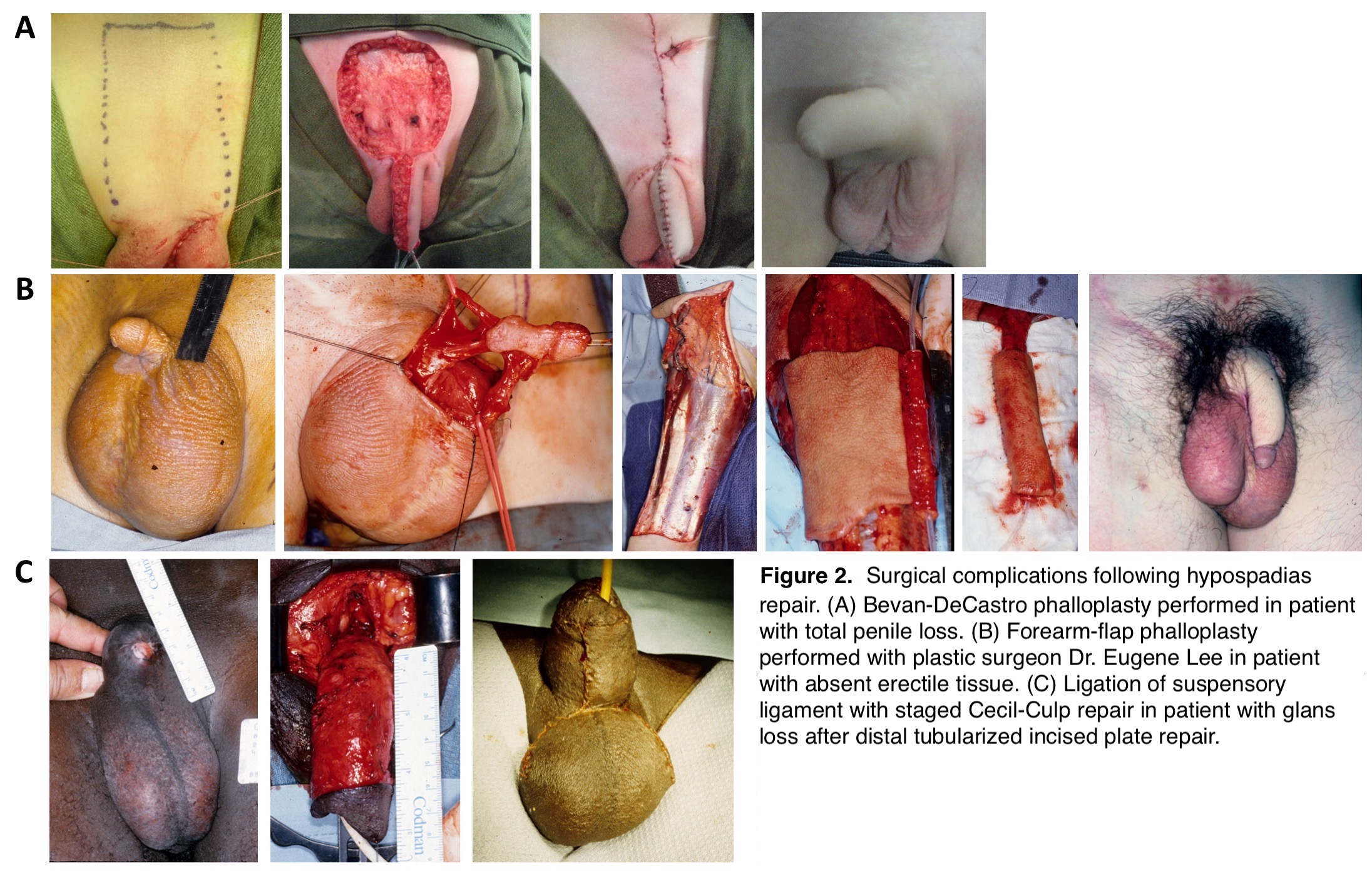
Introduction: Despite the high re-operation rates after proximal hypospadias repairs, surgeons have rarely reported disastrous complications of hypospadias surgery. Herein we report on 16 patients who sustained partial or total glandular or penile loss after hypospadias surgery and were referred to us for further management over the last 40 years (Figure 1). Methods: Operative details of the primary surgery were not available in the majority of cases as six cases were from Egypt, one from Portugal, and one from Iraq. Forty-four percent (7/16) of the index operations utilized epinephrine mixed with local anesthetic. The surgical repairs we performed included Bevan-DeCastro phalloplasty (4), forearm flap phalloplasty (1), and penile lengthening by cutting the suspensory ligament (6) followed by resurfacing using either rotational scrotal flap (3) or staged Cecil-Culp repair (3) [Figure 2]. Four patients underwent contouring of the glans penis. One patient declined treatment. Results: Significant penile lengthening was achieved in all patients ranging from 5 to 8 cm (75-150% of the preoperative penile length). Phalloplasty was technically successful in all patients however we deferred urethroplasty in the four Bevan-DeCastro repairs to a later date during adolescence when forearm flap phalloplasty and penile prosthetic implant are practical. All five phalloplasty patients had acceptable cosmetic result in the absence of erectile function. Conclusions: Partial or total glandular or penile loss subsequent to hypospadias repair is a rare and disastrous complication. Subsequent surgical repair provides some value in improving outcomes. We discourage the use of epinephrine injections during hypospadias repairs and emphasize the importance of leaving the glans exposed to allow for postoperative visual examination and early recognition of vascular compromise. SOURCE OF Funding: None