Urology Physician Resident New York Medical College
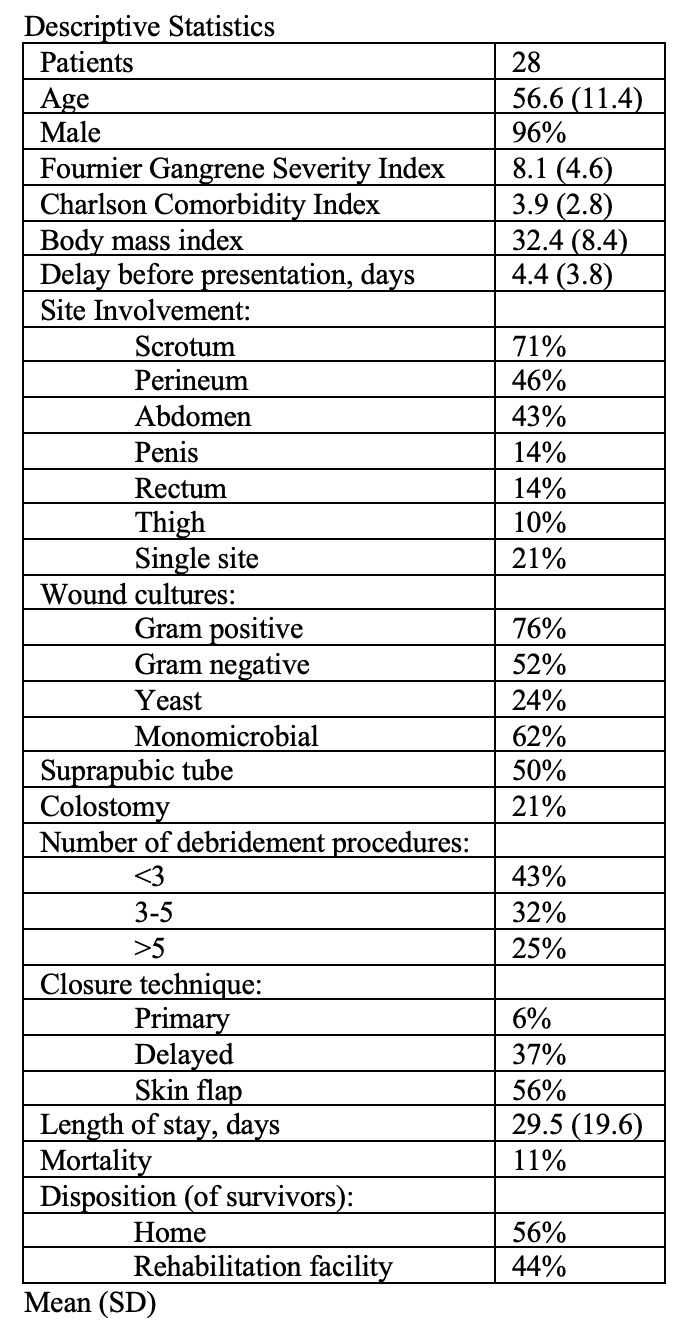
Introduction: Fournier’s Gangrene (FG) is a life-threatening but rare urologic emergency. The prognosis depends on several factors, many of which are captured by the Fournier Gangrene Severity Index (FGSI). We aimed to identify predictors of mortality, prolonged length of stay, and home discharge in a patient sample from a single center over a 11-year period. Methods: Patients treated for FG at a tertiary care facility between 2011-2022 were identified using diagnosis codes and then data from the index hospitalizations were manually extracted. Captured data included demographic and baseline comorbidities, FGSI, operative treatment, and postoperative course and outcomes. Univariate logistic regression analyses were performed for mortality, composite mortality or >6-week length of stay (LOS), and home discharge. Results: Predictors of mortality were FGSI >=14 (ß=3.8, p=0.015) and Charlson comorbidity index (CCI) >=8 (ß=3.1, p=0.028); predictors of composite mortality or >6-week LOS were FGSI >=10 (ß=2.5, p=0.009), delay before presentation >=2 days (ß=-2.4, p=0.046), and abdominal involvement (ß=2.6, p=0.007); and the predictor of home discharge was CCI <4 (ß=3.3, p=0.012). Conclusions: FGSI was an accurate predictor of mortality in this cohort. Baseline health, rather than disease severity, was the strongest predictor of ability to be discharged directly to home. Presentation within one day of symptom onset may indicate fulminant disease and was associated with poor outcomes. Finally, empiric antimicrobial therapy should include antifungal coverage, as Candida species were found in a quarter of wound cultures. SOURCE OF Funding: NA

 photo")