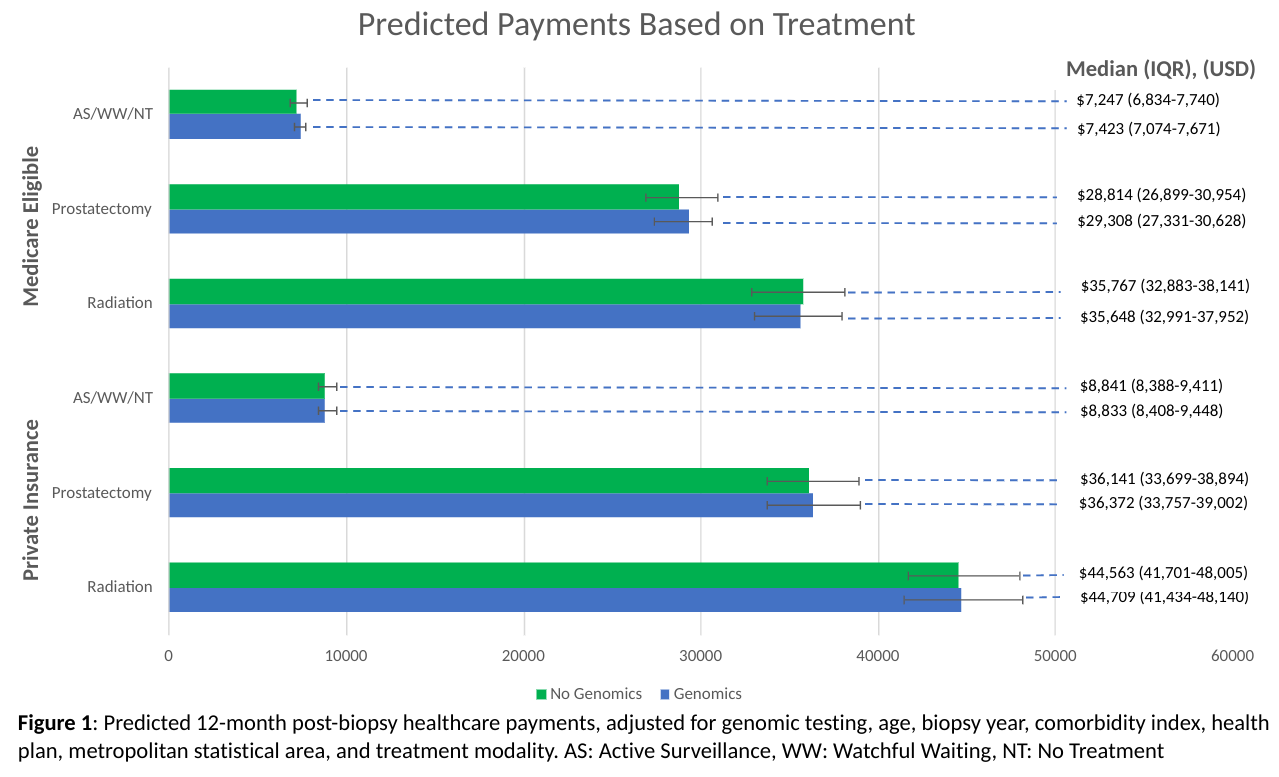
Introduction: Tissue-based genomic biomarkers have been approved for use in risk-stratification of prostate cancer for more than a decade. Prior cost analyses relied on simulation modeling of artificial cohorts, and there has been limited research on real-world expenditures. We assessed 12-month post-biopsy healthcare payments to compare payer expenditures for prostate cancer patients who did and did not receive post-biopsy tissue-based genomic testing. Methods: We used IBM MarketScan Commercial Claims and Medicare Supplemental data to identify newly-diagnosed patients (2018–2019). Inflation-adjusted total healthcare payments were calculated in the 12-month period following diagnostic biopsy. Outliers with the top and bottom 2.5% percentile of total payments were excluded. Multivariable linear regression was conducted to estimate the effect of receiving genomic testing (Oncotype DX, Prolaris, and Decipher) on payments, after controlling for treatment modality, insurance status, and other demographic information. We stratified our analysis based on treatment received. Results: We identified 10,859 patients in our cohort (9,242 privately-insured; 1,617 Medicare eligible). Among this group, 24% received radiation therapy (RT), 44% had radical prostatectomy (RP), and 33% had no identified treatment (AS/WW/NT). Genomic testing was more common in 2019 than 2018 (6.9% vs. 3.5%, p<.001) and was more common in the AS/WW/NT group (8.3%) than those treated with RT (3.4%) or RP (3.9%), p<.001. Median payments for each genomic test ranged from $2,156-3,873. Prediction modeling based on multivariable analysis demonstrated that genomic testing is associated with payment differences ranging from -$119 to +$494 in individual treatment groups (figure 1). Conclusions: Use of tissue-based genomic testing is associated with significant expense. Despite this expense, their use was associated with similar total payments across treatment groups, with the greatest savings ($119) in Medicare patients receiving RT and the greatest expense in Medicare patients undergoing RP ($494). SOURCE OF Funding: None

 photo")