Resident Physician University of Wisconsin School of Medicine and Public Health
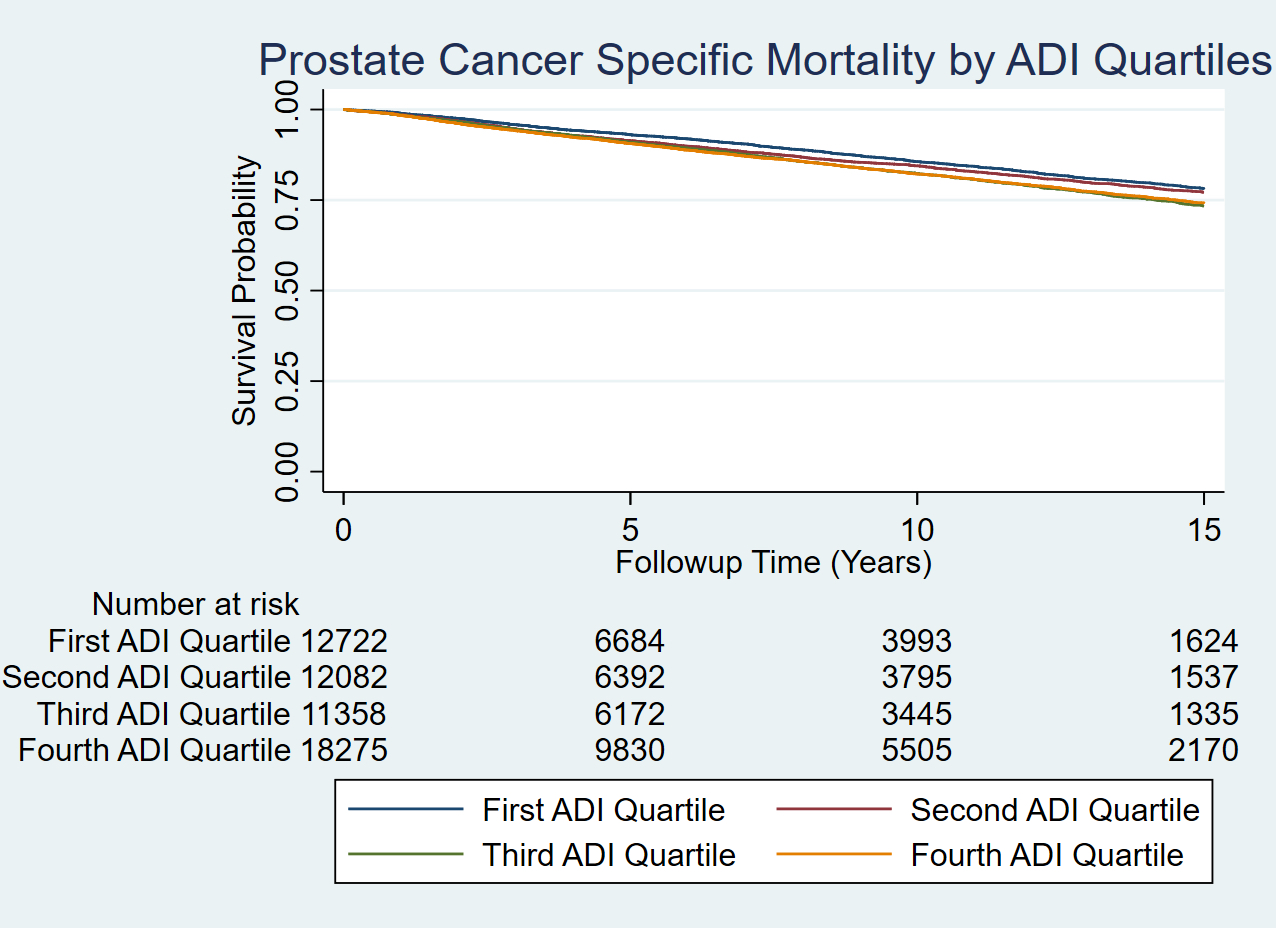
Introduction: Neighborhood deprivation contributes to worsened prostate cancer (PCa) outcomes. In Wisconsin, 54% of the population resides in the most deprived neighborhoods and the state ranks #1 in PCa incidence for Black men. In this study, we aimed to identify the association between neighborhood deprivation, race, and PCa-specific mortality (PCSM) for Wisconsin men. Methods: Wisconsin Cancer Reporting System (WCRS) data were used to identify all men diagnosed with PCa between 1995-2010. Deprivation was measured by the Area of Deprivation Index (ADI) at the census block group level using the Neighborhood Atlas®, a validated composite measure which allows for rankings of neighborhoods by socioeconomic disadvantage based on income, education, employment, and housing quality. ADIs were categorized into quartiles. Differences in baseline demographic and clinicopathologic characteristics were determined using chi-square tests. Cox proportional hazards models were used to estimate the effect of neighborhood deprivation and race on PCSM, adjusted for age, clinical grade, stage, diagnosis year +/- treatment. Results: 62,474 men with PCa were identified including 58,777 White, 2,706 Black, and 991 Other with a median follow up of 5.7 years (primary) and 9.6 years (sensitivity analyses). 33,558 men resided in the most deprived neighborhoods (Q3-Q4): 30,678 White vs 2,282 Black vs 591 Other. PCa-specific deaths were more prevalent in Q4 (12.5%) vs Q1 (9.6%), p<0.001. Men living in the most deprived neighborhoods had a slightly higher risk for PCSM (Q4: [aHR] = 1.1 [95% CI 1.0-1.15], p=0.037). Deprived Black men were at a higher risk of PCSM vs deprived (Q4: HR = 1.2 [95%CI 1.06-1.38], p=0.005) and least deprived White men (HR = 1.3 [95% CI 1.15-1.52], p<0.001), but these were not statistically significant on adjusted and sensitivity analyses (p=0.13-0.88). The least deprived Black men (Q1: aHR= 1.1 [95%CI 0.57-2.05], p=0.79) were no more likely to die from PCa than the least deprived White men. Conclusions: Race is implicated in worsened PCa outcomes, however, these findings support the association between neighborhood deprivation and PCSM as a potential mediator for race effects. These data support that neighborhood-level resources or interventions, such as access to care, are essential to improve or equalize PCa outcomes. SOURCE OF Funding: AUA/UCF Research Scholar Award Grant# 017-822959