Session: PD16: Prostate Cancer: Advanced (including Drug Therapy) III
PD16-03: Prognostic value of Prostate-specific antigen kinetics during treatment of advanced prostate cancer with Abiraterone and Enzalutamide: Multicenter Analysis
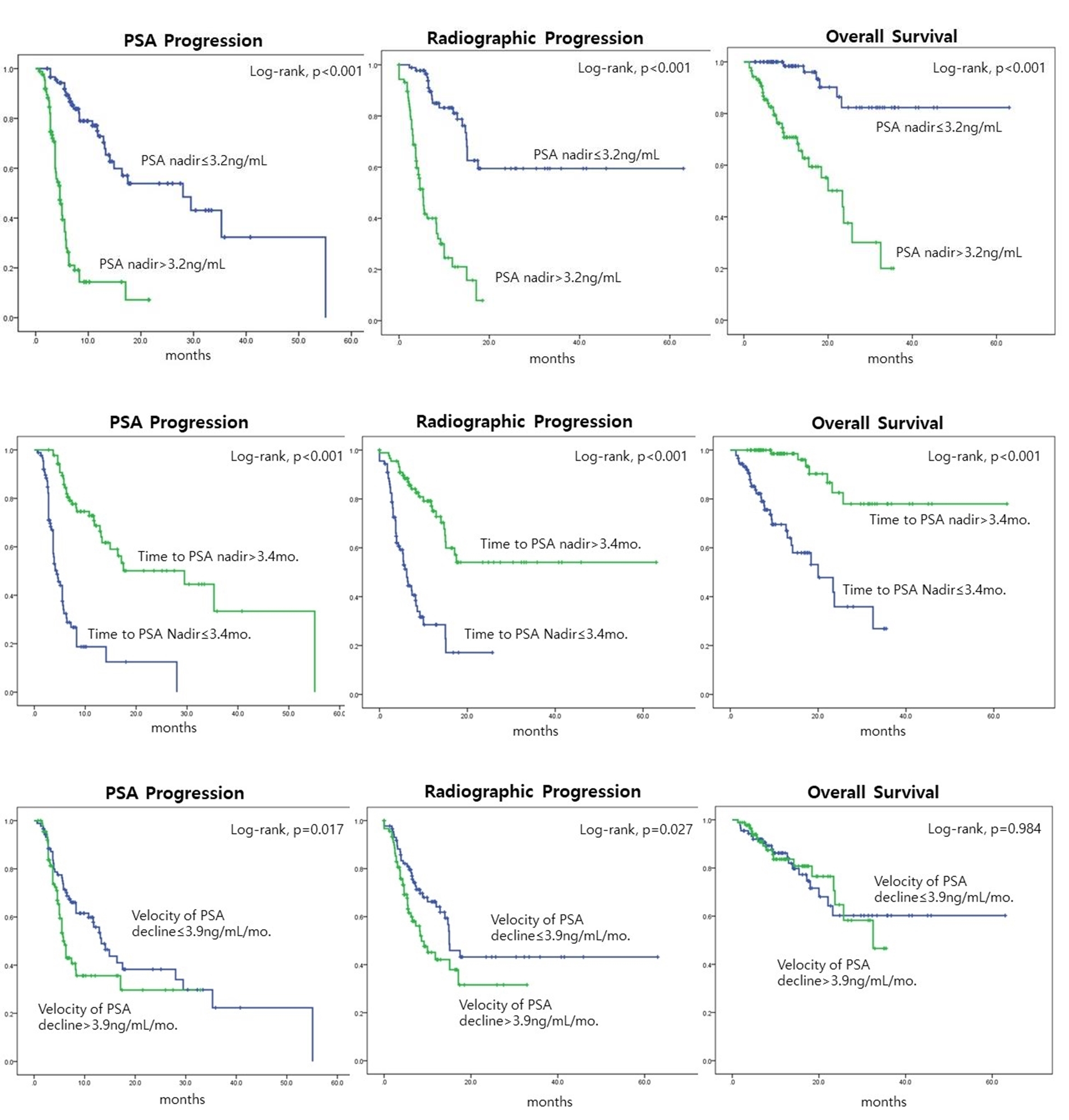
Introduction: This multicenter study aimed to investigate the prognostic value of prostate-specific antigen (PSA) kinetics during the treatment of advanced Prostate Cancer (PCa) with Abiraterone and Enzalutamide. Methods: This multicenter retrospective study evaluated 255 patients with advanced PCa treated with Abiraterone and Enzalutamide between September 2013 and May 2022. All the patients used only one of the two drugs. This study analyzed the following clinical variables: age, clinical TNM stage, Gleason grade, HSPC or CRPC, non-metastatic or metastatic, PSA at the initiation of treatment, Time to PSA nadir, Velocity of PSA decline, and PSA nadir after treatment. We analyzed PSA progression, Radiographic progression-free survival (rPFS), and overall survival (OS) with Kaplan-Meier curves and Cox proportional hazard models. We defined PSA progression, rPFS, and OS based on Prostate Cancer Working Group 2 criteria. Results: The number of patients treated with Abiraterone and Enzalutamide were 94 (36.9%) and 161 (63.1%), respectively. Abiraterone showed a better prognosis than Enzalutamide for PSA progression (log-rank, p<0.05) but not for rPFS and OS (log-rank, p=0.11, and p=0.07). The group with a Time to PSA nadir of 3.4 months or longer had a significantly better prognosis in all of PSA progression, rPFS, and OS (log-rank, p<0.05 for each). The group with the Velocity of PSA decline of 3.9 ng/mL/month or less showed a better prognosis in PSA progression (log-rank, p=0.017) and rPFS (log-rank, p=0.027) but not in OS (log-rank, p=0.984). The group with a PSA nadir of 3.2 ng/mL or less had a better prognosis in all PSA progression, rPFS, and OS (log-rank, p<0.05 for each). In Cox regression analysis, PSA nadir and Time to PSA nadir (p < 0.05, for each) were significant factors for PSA progression, rPFS, and OS, respectively. However, the Velocity of PSA decline was only significantly associated with OS (p < 0.05). Conclusions: In advanced PCa patients treated with Abiraterone and Enzalutamide, PSA kinetics can be a prognostic indicator of progression and OS. Patients with a longer time to nadir, lower PSA nadir, and slower velocity of PSA decline are more likely to have a better prognosis. SOURCE OF Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors