Introduction: Genital tissue loss is a surgical challenge often occurring in complex patients. Scrotoplasty with flaps and split thickness skin grafts (STSG) are two methods of closure but carry complication rates as high as 28% and may not be ideal for medically complex patients. However, closure by secondary intention is associated with wound care needs and patient discomfort. Our objective is to evaluate an alternative method of perineal closure in lieu of scrotoplasty in a complex population. Methods: We retrospectively reviewed patient charts of adults who underwent perineal closure with fasciocutaneous flaps and thigh pouch creation. Our primary outcomes were complication rate and wound coverage. Secondary outcomes included measures of patient satisfaction and post-operative care needs. Results: 20 patients were identified who underwent this closure, the majority following Fourniers gangrene. Patients had a median age of 64 (IQR 58 – 70), BMI of 34 (IQR 29 – 40) and Charlson comorbidity index of 5 (IQR 4 – 8) equating to a 21% 10-year survival. The median total wound dimension was 443 cm2 (IQR 225 – 600). Operative technique in all cases included testicular thigh pouch and fasciocutaneous flap creation from the thigh (n = 18) or abdominal wall (n = 8) and resulted in 100% closure rate of the perineum. Escutcheonectomy was used to increase the size of abdominal flaps in 2 patients with over 600 cm2 of skin loss. Only three patients required abdominal STSG to complete closure. Complication rate was 15% with 1 wound infection and 2 episodes of bleeding. Patients stayed a median of 7.5 days following closure (IQR 3-12.5) and 40% were discharged home. Median follow up was 9 months (n = 16, IQR 3.25 – 14.75) with only 1 patient (6%) reporting pain related to thigh pouches and none desiring elective scrotoplasty. Conclusions: Despite large defects, this method of reconstruction allowed for perineal closure in all patients with minimal use of STSG. Despite significant medical comorbidity, complication rates were comparable to those previously reported and patients were largely satisfied with their reconstruction with none desiring formal scrotoplasty. While larger sample sizes are needed, this method of closure appears to add an option for the medically and surgically complex perineal reconstruction patient. SOURCE OF Funding: None

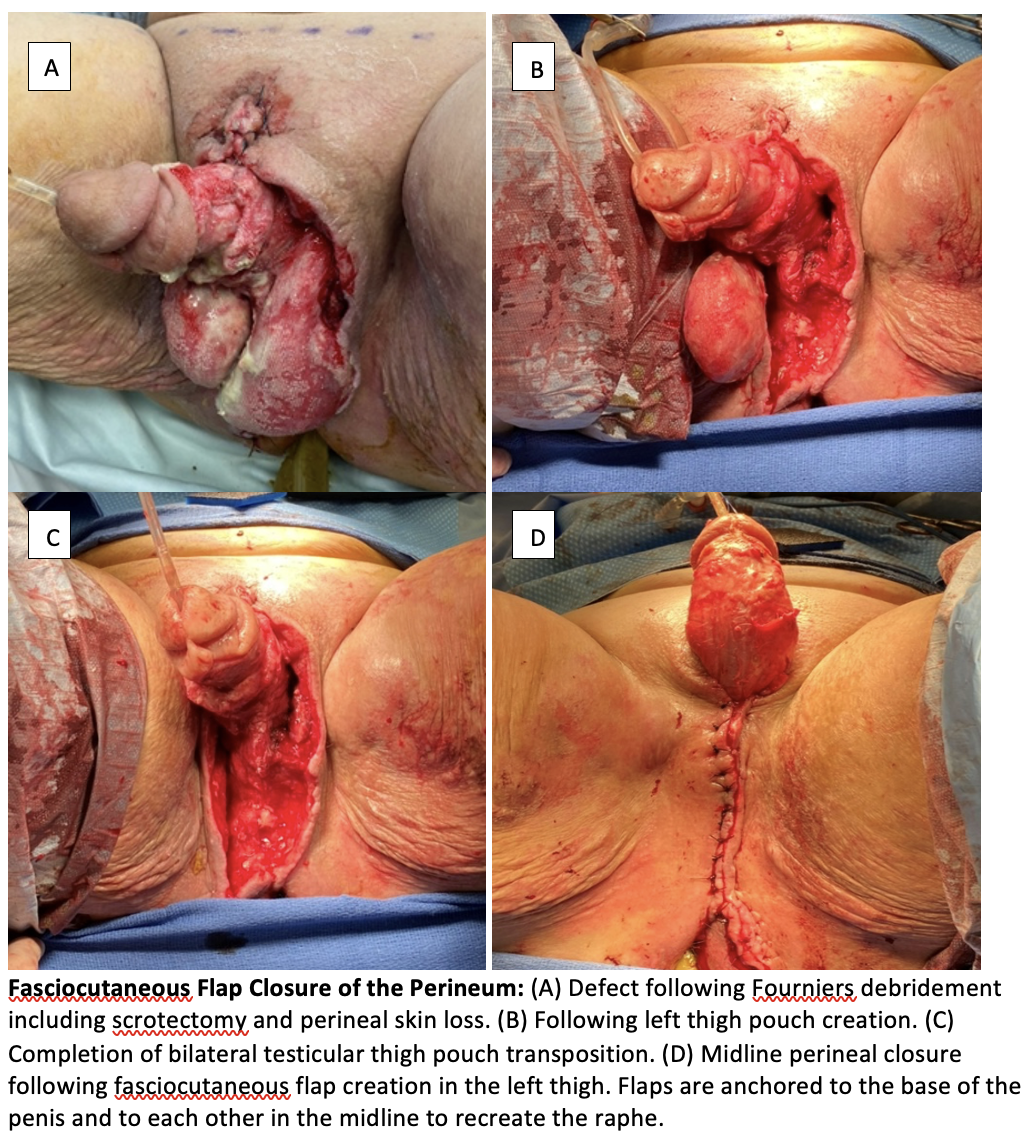
 photo")